

Influenza aerosols in UK hospitals during the H1N1 (2009) pandemic--the risk of aerosol generation during medical procedures
- PMID: 23418548
- PMCID: PMC3571988
- DOI: 10.1371/journal.pone.0056278
Influenza aerosols in UK hospitals during the H1N1 (2009) pandemic--the risk of aerosol generation during medical procedures
Abstract
Background: Nosocomial infection of health-care workers (HCWs) during outbreaks of respiratory infections (e.g. Influenza A H1N1 (2009)) is a significant concern for public health policy makers. World Health Organization (WHO)-defined 'aerosol generating procedures' (AGPs) are thought to increase the risk of aerosol transmission to HCWs, but there are presently insufficient data to quantify risk accurately or establish a hierarchy of risk-prone procedures.
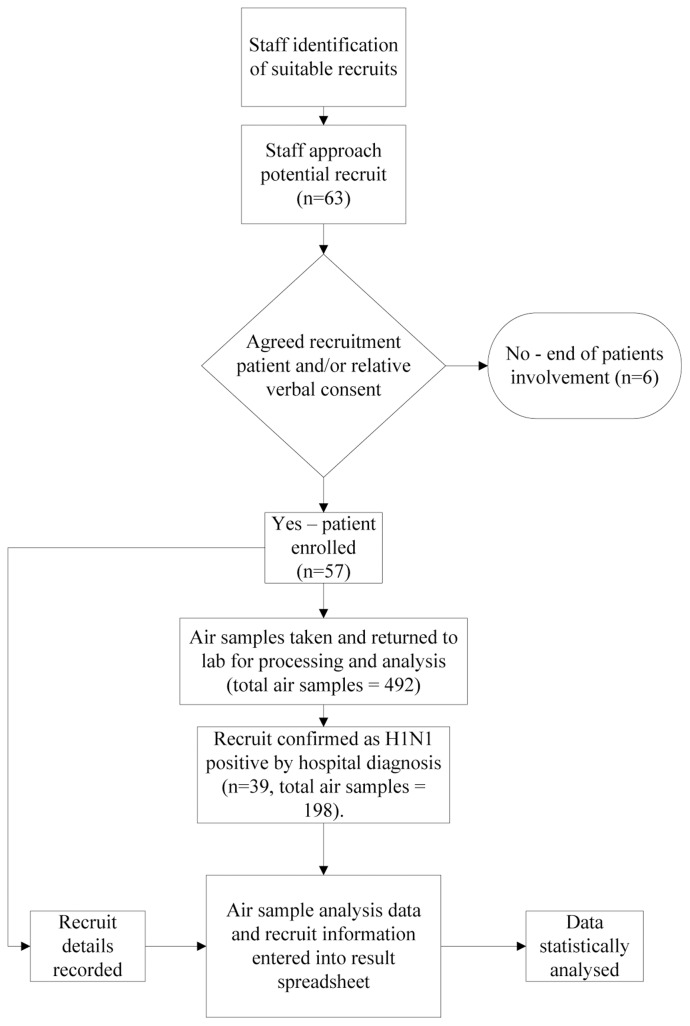
Methodology/principal findings: This study measured the amount of H1N1 (2009) RNA in aerosols in the vicinity of H1N1 positive patients undergoing AGPs to help quantify the potential risk of transmission to HCWs. There were 99 sampling occasions (windows) producing a total of 198 May stages for analysis in the size ranges 0.86-7.3 µm. Considering stages 2 (4-7.3 µm) and 3 (0.86-4 µm) as comprising one sample, viral RNA was detected in 14 (14.1%) air samples from 10 (25.6%) patients. Twenty three air samples were collected while potential AGPs were being performed of which 6 (26.1%) contained viral RNA; in contrast, 76 May samples were collected when no WHO 2009 defined AGP was being performed of which 8 (10.5%) contained viral RNA (unadjusted OR = 2.84 (95% CI 1.11-7.24) adjusted OR = 4.31 (0.83-22.5)).
Conclusions/significance: With our small sample size we found that AGPs do not significantly increase the probability of sampling an H1N1 (2009) positive aerosol (OR (95% CI) = 4.31 (0.83-22.5). Although the probability of detecting positive H1N1 (2009) positive aerosols when performing various AGPs on intensive care patients above the baseline rate (i.e. in the absence of AGPs) did not reach significance, there was a trend towards hierarchy of AGPs, placing bronchoscopy and respiratory and airway suctioning above baseline (background) values. Further, larger studies are required but these preliminary findings may be of benefit to infection control teams.
Conflict of interest statement
Figures
Similar articles
-
Virus shedding and environmental deposition of novel A (H1N1) pandemic influenza virus: interim findings.Health Technol Assess. 2010 Oct;14(46):237-354. doi: 10.3310/hta14460-04. Health Technol Assess. 2010. PMID: 20923613
-
Exposure to influenza virus aerosols during routine patient care.J Infect Dis. 2013 Apr;207(7):1037-46. doi: 10.1093/infdis/jis773. Epub 2013 Jan 30. J Infect Dis. 2013. PMID: 23372182
-
Evaluation of droplet dispersion during non-invasive ventilation, oxygen therapy, nebuliser treatment and chest physiotherapy in clinical practice: implications for management of pandemic influenza and other airborne infections.Health Technol Assess. 2010 Oct;14(46):131-172. doi: 10.3310/hta14460-02. Health Technol Assess. 2010. PMID: 20923611
-
Current Insights Into Respiratory Virus Transmission and Potential Implications for Infection Control Programs : A Narrative Review.Ann Intern Med. 2021 Dec;174(12):1710-1718. doi: 10.7326/M21-2780. Epub 2021 Nov 9. Ann Intern Med. 2021. PMID: 34748374 Review.
-
Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review.PLoS One. 2012;7(4):e35797. doi: 10.1371/journal.pone.0035797. Epub 2012 Apr 26. PLoS One. 2012. PMID: 22563403 Free PMC article. Review.
Cited by
-
[Recommendations for therapy in pandemic times: Acting (and treating) correctly under pressure to act].Notf Rett Med. 2020;23(5):382-384. doi: 10.1007/s10049-020-00739-y. Epub 2020 Jul 14. Notf Rett Med. 2020. PMID: 32837304 Free PMC article. German. No abstract available.
-
The use of pediatric flexible bronchoscopy in the COVID-19 pandemic era.Pediatr Pulmonol. 2021 Jul;56(7):1957-1966. doi: 10.1002/ppul.25358. Epub 2021 Mar 17. Pediatr Pulmonol. 2021. PMID: 33730395 Free PMC article. Review.
-
Validation and application of models to predict facemask influenza contamination in healthcare settings.Risk Anal. 2014 Aug;34(8):1423-34. doi: 10.1111/risa.12185. Epub 2014 Mar 4. Risk Anal. 2014. PMID: 24593662 Free PMC article.
-
Mechanistic theory predicts the effects of temperature and humidity on inactivation of SARS-CoV-2 and other enveloped viruses.Elife. 2021 Jul 13;10:e65902. doi: 10.7554/eLife.65902. Elife. 2021. PMID: 33904403 Free PMC article.
-
Potential for occupational exposures to pathogens during bronchoscopy procedures.J Occup Environ Hyg. 2019 Oct;16(10):707-716. doi: 10.1080/15459624.2019.1649414. Epub 2019 Aug 13. J Occup Environ Hyg. 2019. PMID: 31407954 Free PMC article.
References
-
- Booth CM, Matukas LM, Tomlinson GA, Rachlis AR, Rose DB, et al. (2003) Clinical features and short-term outcomes of 144 patients with SARS in the greater Toronto area. JAMA 289: 2801–2809. - PubMed
-
- CDC (2003) Severe acute respiratory syndrome–Taiwan, 2003. MMWR Morb Mortal Wkly Rep 52: 461–466. - PubMed
-
- Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J (2012) Aerosol Generating Procedures and Risk of Transmission of Acute Respiratory Infections to Healthcare Workers: A Systematic Review. PLoS ONE 7(4): e35797 doi:10.1371/journal.pone.0035797. - DOI - PMC - PubMed
-
- Davies A, Thomson G, Walker J, Bennett AM (2009) A review of the risks and disease transmission associated with aerosol generating medical procedures. Journal of Infection Prevention 10: 122–126.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
