

Recent progress in the pathophysiology and treatment of FSGS recurrence
- PMID: 23312002
- PMCID: PMC3558619
- DOI: 10.1111/ajt.12045
Recent progress in the pathophysiology and treatment of FSGS recurrence
Abstract
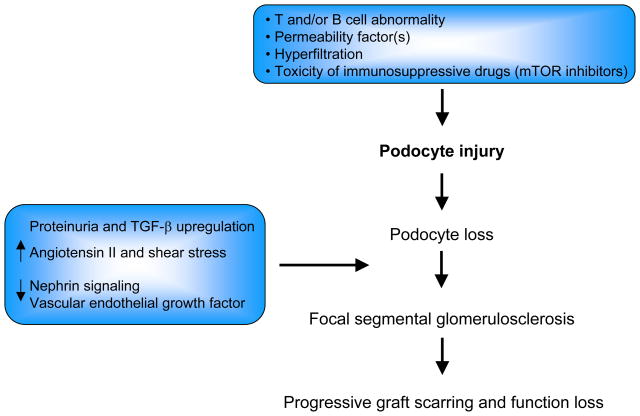
Focal segmental glomerulosclerosis (FSGS) is a glomerular disease characterized by proteinuria, frequent progression to end-stage renal disease, and recurrence after kidney transplantation in ∼25% of patients, which negatively impacts long-term allograft survival. Experimental studies suggest that abnormalities in T and, possibly, B cells may represent one initial pathogenic trigger, leading to podocyte injury and progressive loss. New data also support the existence of circulating permeability factors able to damage the podocytes, but no single molecule has been consistently identified as the causal pathogenic element in FSGS recurrence. Unfortunately, major progress from mechanistic studies has not translated into substantial advancements in patient treatment, with plasmapheresis (PP) and high doses of cyclosporine (CsA) remaining the mainstays of therapy. Despite consistent experimental and clinical evidence that treatment of proteinuria slows renal function decline in proteinuric nephropathies, maximal use of antiproteinuric agents such as renin angiotensin system antagonists is not routine in the management of FSGS recurrence. More recently, encouraging results have been reported with anti-CD20 depleting antibody rituximab, but further studies are needed to establish its safety/efficacy profile.
© Copyright 2013 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to disclose as described by the American Journal of Transplantation.
Figures
Similar articles
-
Rituximab targets podocytes in recurrent focal segmental glomerulosclerosis.Sci Transl Med. 2011 Jun 1;3(85):85ra46. doi: 10.1126/scitranslmed.3002231. Sci Transl Med. 2011. PMID: 21632984 Free PMC article.
-
FSGS Recurrence in Adults after Renal Transplantation.Biomed Res Int. 2016;2016:3295618. doi: 10.1155/2016/3295618. Epub 2016 Apr 10. Biomed Res Int. 2016. PMID: 27144163 Free PMC article. Review.
-
Prediction and treatment of recurrent focal segmental glomerulosclerosis after renal transplantation in children.Am J Kidney Dis. 1999 Dec;34(6):1048-55. doi: 10.1016/S0272-6386(99)70010-7. Am J Kidney Dis. 1999. PMID: 10585314
-
Success with plasmapheresis treatment for recurrent focal segmental glomerulosclerosis in pediatric renal transplant recipients.Pediatr Transplant. 2014 Feb;18(1):29-34. doi: 10.1111/petr.12185. Epub 2013 Nov 25. Pediatr Transplant. 2014. PMID: 24266922
-
Recurrence of focal-segmental glomerulosclerosis in children after renal transplantation: clinical and genetic aspects.Transplantation. 2005 Sep 27;80(1 Suppl):S128-34. doi: 10.1097/01.tp.0000187110.25512.82. Transplantation. 2005. PMID: 16286890 Review.
Cited by
-
The importance of non-HLA antibodies in transplantation.Nat Rev Nephrol. 2016 Aug;12(8):484-95. doi: 10.1038/nrneph.2016.88. Epub 2016 Jun 27. Nat Rev Nephrol. 2016. PMID: 27345243 Free PMC article. Review.
-
Circulating and urinary microRNA profile in focal segmental glomerulosclerosis: a pilot study.Eur J Clin Invest. 2015 Apr;45(4):394-404. doi: 10.1111/eci.12420. Eur J Clin Invest. 2015. PMID: 25682967 Free PMC article.
-
Therapeutic apheresis in kidney transplantation: An updated review.World J Transplant. 2019 Oct 28;9(6):103-122. doi: 10.5500/wjt.v9.i6.103. World J Transplant. 2019. PMID: 31750088 Free PMC article. Review.
-
LDL-apheresis-induced remission of focal segmental glomerulosclerosis recurrence in pediatric renal transplant recipients.Pediatr Nephrol. 2019 Nov;34(11):2343-2350. doi: 10.1007/s00467-019-04296-6. Epub 2019 Jun 27. Pediatr Nephrol. 2019. PMID: 31250206
-
Update on the treatment of focal segmental glomerulosclerosis in renal transplantation.World J Transplant. 2016 Mar 24;6(1):54-68. doi: 10.5500/wjt.v6.i1.54. World J Transplant. 2016. PMID: 27011905 Free PMC article. Review.
References
-
- Gallon L, Leventhal J, Skaro A, Kanwar Y, Alvarado A. Resolution of recurrent focal segmental glomerulosclerosis after retransplantation. N Engl J Med. 2012;366(17):1648–1649. - PubMed
-
- McGrogan A, Franssen CF, de Vries CS. The incidence of primary glomerulonephritis worldwide: a systematic review of the literature. Nephrol Dial Transplant. 2011;26(2):414–430. - PubMed
-
- Kitiyakara C, Eggers P, Kopp JB. Twenty-one-year trend in ESRD due to focal segmental glomerulosclerosis in the United States. Am J Kidney Dis. 2004;44(5):815–825. - PubMed
-
- Kitiyakara C, Kopp JB, Eggers P. Trends in the epidemiology of focal segmental glomerulosclerosis. Semin Nephrol. 2003;23(2):172–182. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
