

Estimation of HIV-testing rates to maximize early diagnosis-derived benefits at the individual and population level
- PMID: 23308161
- PMCID: PMC3538781
- DOI: 10.1371/journal.pone.0053193
Estimation of HIV-testing rates to maximize early diagnosis-derived benefits at the individual and population level
Abstract
Background: In HIV infection, initiation of treatment is associated with improved clinical outcom and reduced rate of sexual transmission. However, difficulty in detecting infection in early stages impairs those benefits. We determined the minimum testing rate that maximizes benefits derived from early diagnosis.
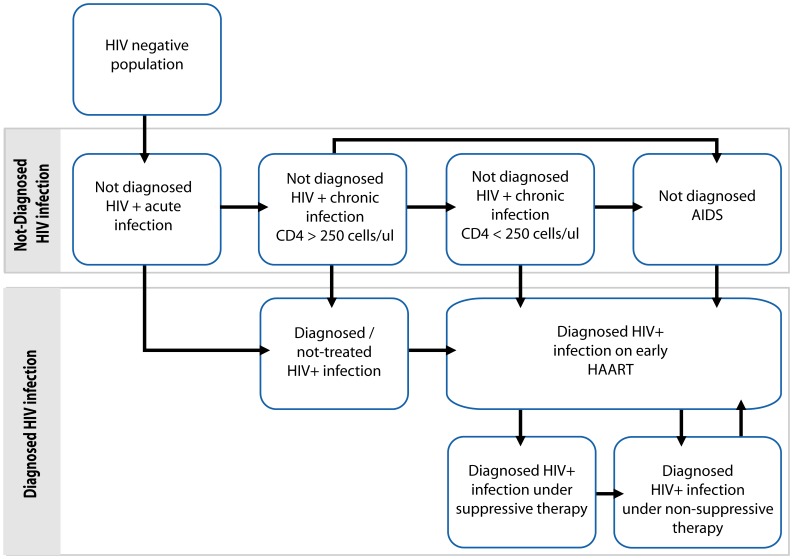
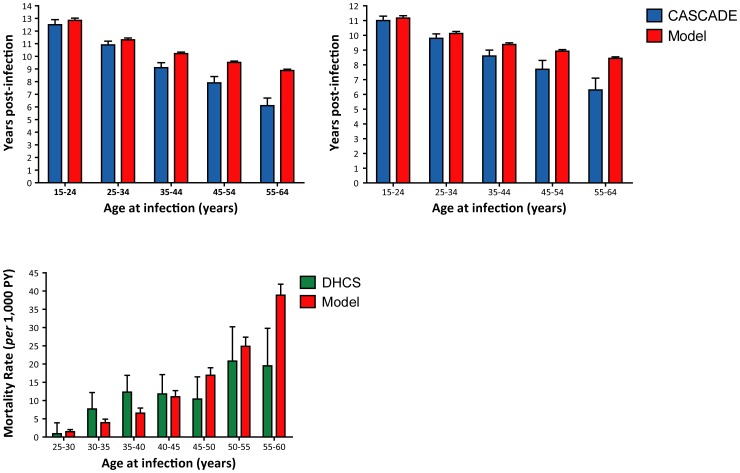
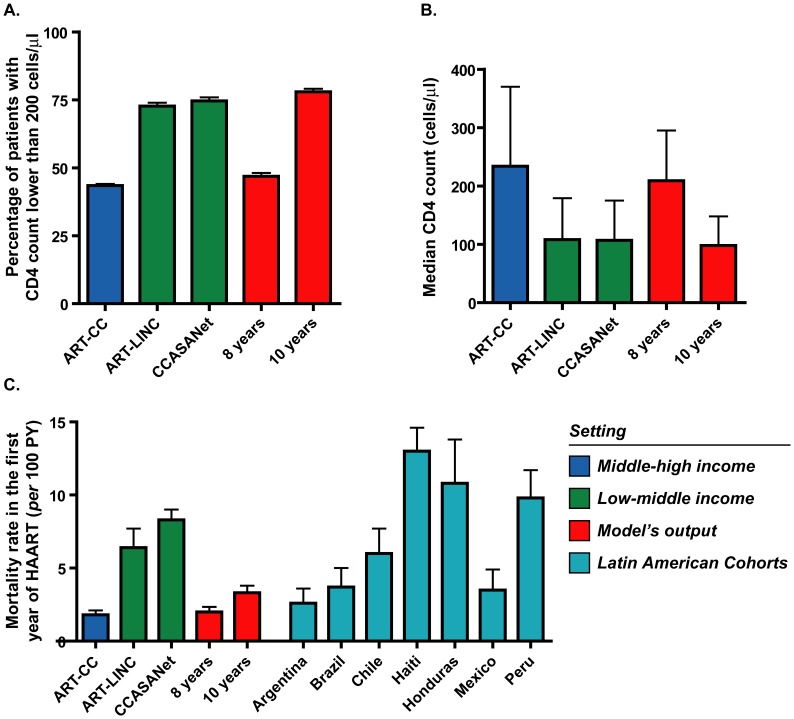
Methods: We developed a mathematical model of HIV infection, diagnosis and treatment that allows studying both diagnosed and undiagnosed populations, as well as determining the impact of modifying time to diagnosis and testing rates. The model's external consistency was assessed by estimating time to AIDS and death in absence of treatment as well as by estimating age-dependent mortality rates during treatment, and comparing them with data previously reported from CASCADE and DHCS cohorts.
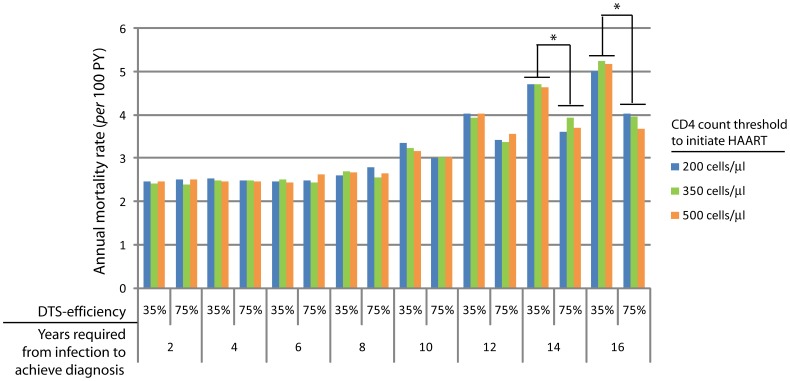
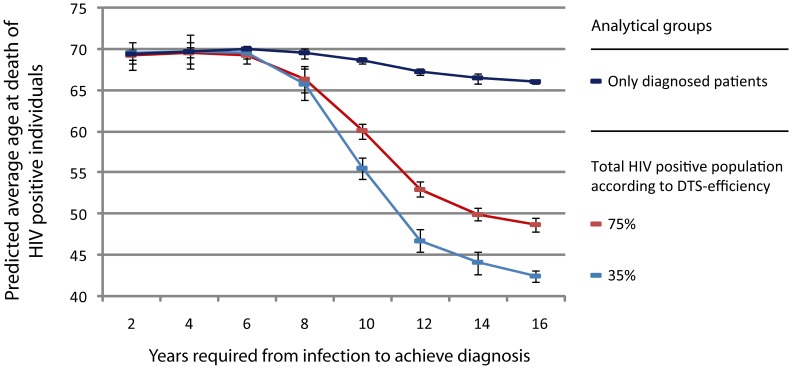
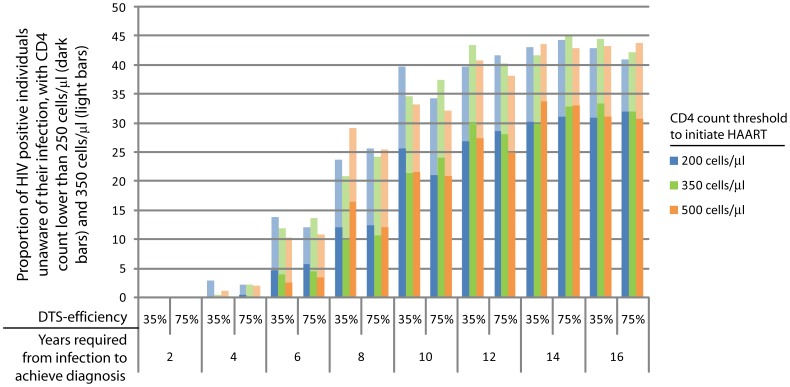
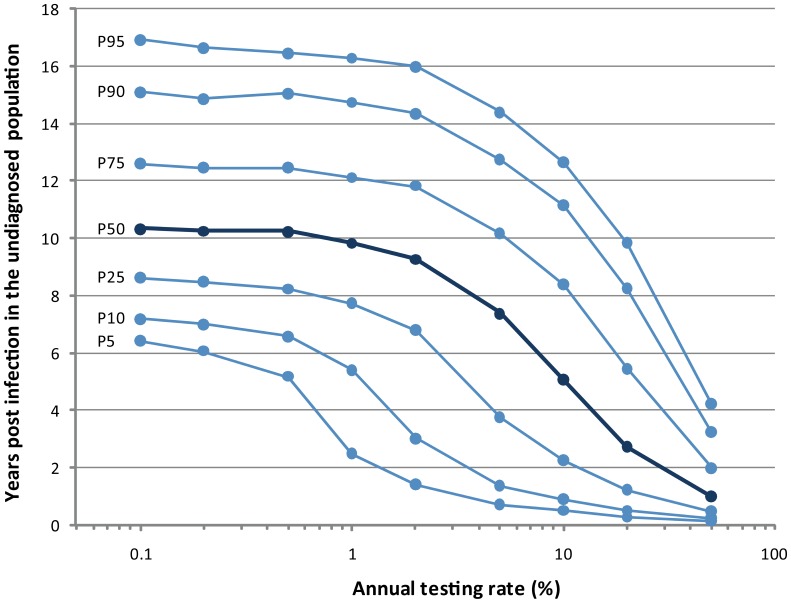
Results: In our model, life expectancy of patients diagnosed before 8 years post infection is the same as HIV-negative population. After this time point, age at death is significantly dependent on diagnosis delay but initiation of treatment increases life expectancy to similar levels as HIV-negative population. Early mortality during HAART is dependent on treatment CD4 threshold until 6 years post infection and becomes dependent on diagnosis delay after 6 years post infection. By modifying testing rates, we estimate that an annual testing rate of 20% leads to diagnosis of 90% of infected individuals within the first 8.2 years of infection and that current testing rate in middle-high income settings stands close to 10%. In addition, many differences between low-income and middle-high incomes can be predicted by solely modifying the diagnosis delay.
Conclusions: To increase testing rate of undiagnosed HIV population by two-fold in middle-high income settings will minimize early mortality during initiation of treatment and global mortality rate as well as maximize life expectancy. Our results highlight the impact of achieving early diagnosis and the importance of strongly work on improving HIV testing rates.
Conflict of interest statement
Figures

Similar articles
-
[The importance of early diagnosis for the survival of HIV positive patients].Medicina (B Aires). 2010;70(5):453-6. Medicina (B Aires). 2010. PMID: 20920966 Spanish.
-
When to start antiretroviral therapy in resource-limited settings.Ann Intern Med. 2009 Aug 4;151(3):157-66. doi: 10.7326/0003-4819-151-3-200908040-00138. Epub 2009 Jul 20. Ann Intern Med. 2009. PMID: 19620143 Free PMC article.
-
Projected life expectancy of people with HIV according to timing of diagnosis.AIDS. 2012 Jan 28;26(3):335-43. doi: 10.1097/QAD.0b013e32834dcec9. AIDS. 2012. PMID: 22089374
-
Tuberculosis.In: Holmes KK, Bertozzi S, Bloom BR, Jha P, editors. Major Infectious Diseases. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 3. Chapter 11. In: Holmes KK, Bertozzi S, Bloom BR, Jha P, editors. Major Infectious Diseases. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 3. Chapter 11. PMID: 30212088 Free Books & Documents. Review.
-
The road to success. Long-term prognosis for persons living with HIV in Denmark - time trends and risk factors.Dan Med J. 2016 Feb;63(2):B5210. Dan Med J. 2016. PMID: 26836803 Review.
Cited by
-
Evaluation of Different Parameters of Humoral and Cellular Immune Responses in HIV Serodiscordant Heterosexual Couples: Humoral Response Potentially Implicated in Modulating Transmission Rates.EBioMedicine. 2017 Dec;26:25-37. doi: 10.1016/j.ebiom.2017.11.001. Epub 2017 Nov 3. EBioMedicine. 2017. PMID: 29129698 Free PMC article.
-
The effect of a local change team intervention on staff attitudes towards HIV service delivery in correctional settings: a randomized trial.AIDS Educ Prev. 2014 Oct;26(5):411-28. doi: 10.1521/aeap.2014.26.5.411. AIDS Educ Prev. 2014. PMID: 25299806 Free PMC article. Clinical Trial.
-
Correlates of Undiagnosed HIV Infection and Retesting Among Voluntary HIV Testing Clients at Mildmay Clinic, Uganda.AIDS Behav. 2019 Apr;23(4):820-834. doi: 10.1007/s10461-018-2274-3. AIDS Behav. 2019. PMID: 30255386 Free PMC article.
-
Epidemiological, clinical, and immunological profile of cases at the time of HIV testing (a clinic-based observational cross-sectional study).Indian J Sex Transm Dis AIDS. 2018 Jan-Jun;39(1):7-12. doi: 10.4103/ijstd.IJSTD_20_18. Indian J Sex Transm Dis AIDS. 2018. PMID: 30187019 Free PMC article.
-
Levels of alcohol use and history of HIV testing among female sex workers in Mombasa, Kenya.AIDS Care. 2014;26(12):1619-24. doi: 10.1080/09540121.2014.938013. Epub 2014 Jul 21. AIDS Care. 2014. PMID: 25040114 Free PMC article.
References
-
- Lohse N, Hansen AB, Pedersen G, Kronborg G, Gerstoft J, et al. (2007) Survival of persons with and without HIV infection in Denmark, 1995–2005. Ann Intern Med 146: 87–95. - PubMed
-
- Mocroft A, Ledergerber B, Katlama C, Kirk O, Reiss P, et al. (2003) Decline in the AIDS and death rates in the EuroSIDA study: an observational study. Lancet 362: 22–29. - PubMed
-
- Mocroft A, Phillips AN, Gatell J, Ledergerber B, Fisher M, et al. (2007) Normalisation of CD4 counts in patients with HIV-1 infection and maximum virological suppression who are taking combination antiretroviral therapy: an observational cohort study. Lancet 370: 407–413. - PubMed
-
- Mocroft A, Vella S, Benfield TL, Chiesi A, Miller V, et al. (1998) Changing patterns of mortality across Europe in patients infected with HIV-1. EuroSIDA Study Group. Lancet 352: 1725–1730. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
