

Effects of coexisting pneumonia and end-stage renal disease on pleural fluid analysis in patients with hydrostatic pleural effusion
- PMID: 23288037
- PMCID: PMC3673666
- DOI: 10.1378/chest.12-2221
Effects of coexisting pneumonia and end-stage renal disease on pleural fluid analysis in patients with hydrostatic pleural effusion
Abstract
Background: In individual patients, especially those who are hospitalized, several conditions often coexist that may be responsible for the development of a pleural effusion and may affect the pleural fluid analysis (PFA). The objective of this study was to investigate the effects of end-stage renal disease and pneumonia on PFA in patients with hydrostatic pleural effusion.
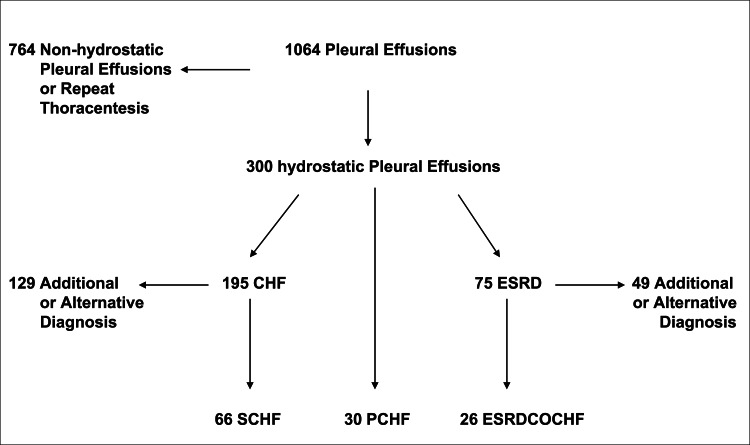
Methods: In a retrospective analysis of 1,064 consecutive patients who underwent thoracentesis at a university hospital, cell counts and pleural fluid protein, lactate dehydrogenase, pH, and glucose levels were examined in those (n = 300) with clinical evidence of hydrostatic pleural effusion.
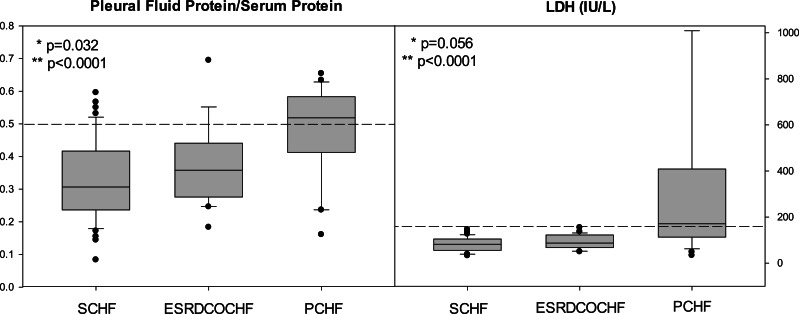
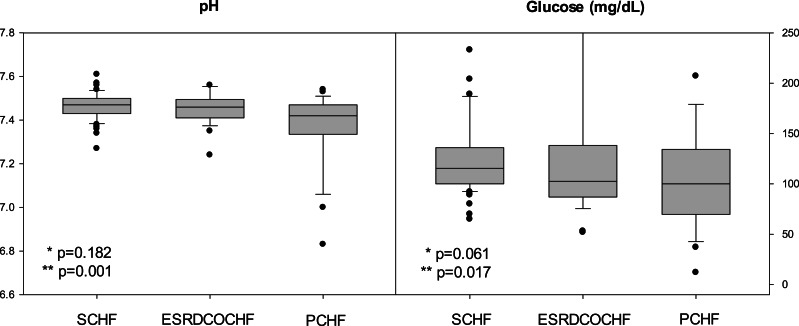
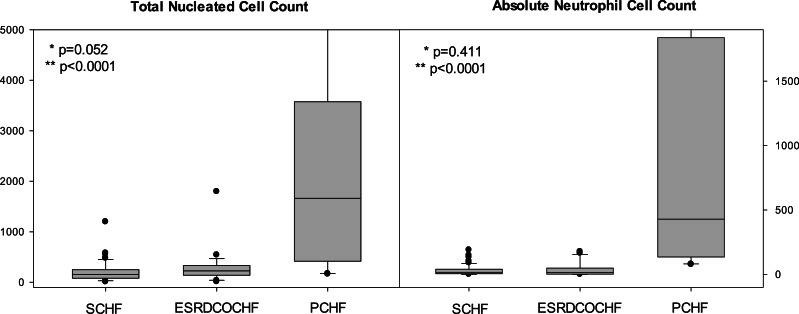
Results: The 300 patients (28.1%) with pleural effusions had congestive heart failure (CHF), circulatory overload (CO), or both. Expert consensus was achieved in 66 (22%) for CHF as the sole diagnosis (SCHF), 30 (10%) for CHF and coexisting pneumonia (PCHF), and 26 (8.7%) for end-stage renal disease (ESRD) with coexisting CO or CHF. The remaining 178 patients were excluded because of complicating conditions. There were minor, but statistically significant differences in pleural fluid/serum protein ratios in patients with ESRD with coexisting CO or CHF compared with SCHF. Compared with SCHF, there were statistically significant tendencies for higher protein and lactate dehydrogenase concentrations and lower pH levels in those with PCHF. The total nucleated cell count and the absolute neutrophil count were significantly higher in PCHF.
Conclusions: ESRD in patients with hydrostatic pleural effusions has a minimal effect on the PFA. Coexisting pneumonia most often results in an exudative effusion in patients with CHF.
Figures
Similar articles
-
Exudative effusions in congestive heart failure.Chest. 2002 Nov;122(5):1518-23. doi: 10.1378/chest.122.5.1518. Chest. 2002. PMID: 12426246
-
Serum and pleural fluid N-Terminal-Pro-B-Type natriuretic peptide concentrations in the differential diagnosis of pleural effusions.Tuberk Toraks. 2011;59(1):1-7. Tuberk Toraks. 2011. PMID: 21554224
-
Influence of diuretics on the concentration of proteins and other components of pleural transudates in patients with heart failure.Am J Med. 2001 Jun 15;110(9):681-6. doi: 10.1016/s0002-9343(01)00726-4. Am J Med. 2001. PMID: 11403751 Clinical Trial.
-
[Contribution of pleural fluid analysis to the diagnosis of pleural effusion].Med Clin (Barc). 2015 Aug 21;145(4):171-7. doi: 10.1016/j.medcli.2014.08.005. Epub 2014 Nov 27. Med Clin (Barc). 2015. PMID: 25433793 Review. Spanish.
-
The differential diagnosis of pleural effusions.West J Med. 1982 Aug;137(2):99-108. West J Med. 1982. PMID: 6182697 Free PMC article. Review.
Cited by
-
Integrative classification of human coding and noncoding genes through RNA metabolism profiles.Nat Struct Mol Biol. 2017 Jan;24(1):86-96. doi: 10.1038/nsmb.3325. Epub 2016 Nov 21. Nat Struct Mol Biol. 2017. PMID: 27870833
-
Clinical characteristics and prognostic factors of non-malignant pleural effusions in hospitalised patients: a retrospective cohort study.BMJ Open. 2024 Jul 30;14(7):e077980. doi: 10.1136/bmjopen-2023-077980. BMJ Open. 2024. PMID: 39079916 Free PMC article.
-
Pleural effusion portends a poor prognosis in patients on continuous ambulatory peritoneal dialysis.PLoS One. 2024 Jan 19;19(1):e0297343. doi: 10.1371/journal.pone.0297343. eCollection 2024. PLoS One. 2024. PMID: 38241413 Free PMC article.
References
-
- Eid AA, Keddissi JI, Samaha M, Tawk MM, Kimmell K, Kinasewitz GT. Exudative effusions in congestive heart failure. Chest. 2002;122(5):1518-1523 - PubMed
-
- Noppen M, De Waele M, Li R, et al. Volume and cellular content of normal pleural fluid in humans examined by pleural lavage. Am J Respir Crit Care Med. 2000;162(3 pt 1):1023-1026 - PubMed
-
- Porcel JM. Establishing a diagnosis of pleural effusion due to heart failure. Respirology. 2009;14(4):471-473 - PubMed
-
- Pillay VK. Total proteins in serous fluids in cardiac failure. S Afr Med J. 1965;39:142-143 - PubMed
-
- Peterman TA, Brothers SK. Pleural effusions in congestive heart failure and in pericardial disease. N Engl J Med. 1983;309(5):313. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
