

Antiretroviral therapy outcomes among adolescents and youth in rural Zimbabwe
- PMID: 23285204
- PMCID: PMC3527625
- DOI: 10.1371/journal.pone.0052856
Antiretroviral therapy outcomes among adolescents and youth in rural Zimbabwe
Abstract
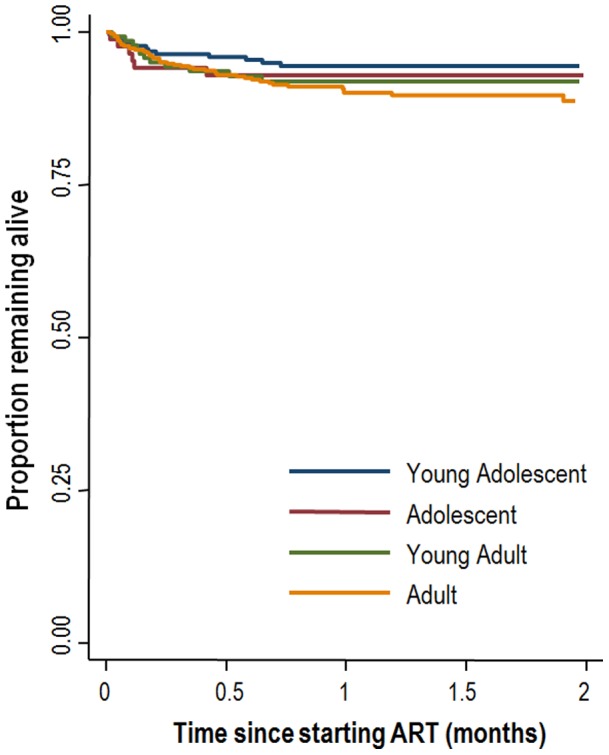
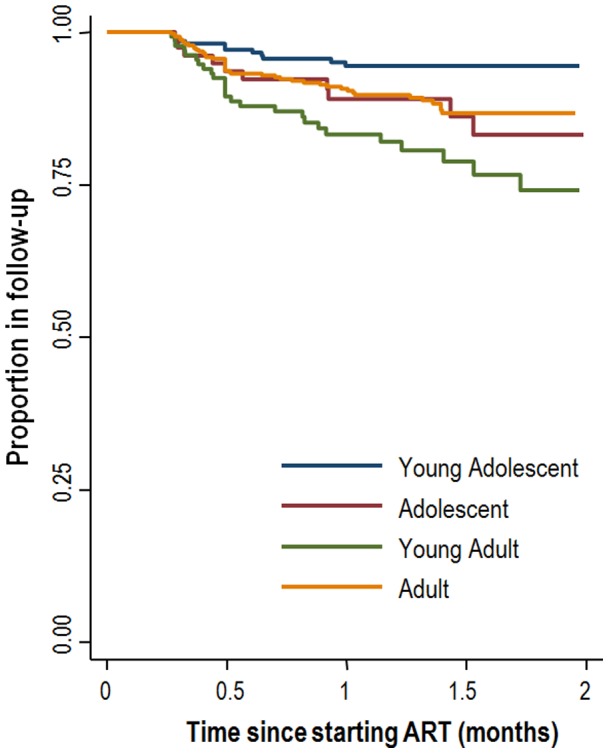
Around 2 million adolescents and 3 million youth are estimated to be living with HIV worldwide. Antiretroviral outcomes for this group appear to be worse compared to adults. We report antiretroviral therapy outcomes from a rural setting in Zimbabwe among patients aged 10-30 years who were initiated on ART between 2005 and 2008. The cohort was stratified into four age groups: 10-15 (young adolescents) 15.1-19 years (adolescents), 19.1-24 years (young adults) and 24.1-29.9 years (older adults). Survival analysis was used to estimate rates of deaths and loss to follow-up stratified by age group. Endpoints were time from ART initiation to death or loss to follow-up. Follow-up of patients on continuous therapy was censored at date of transfer, or study end (31 December 2008). Sex-adjusted Cox proportional hazards models were used to estimate hazard ratios for different age groups. 898 patients were included in the analysis; median duration on ART was 468 days. The risk of death were highest in adults compared to young adolescents (aHR 2.25, 95%CI 1.17-4.35). Young adults and adolescents had a 2-3 times higher risk of loss to follow-up compared to young adolescents. When estimating the risk of attrition combining loss to follow-up and death, young adults had the highest risk (aHR 2.70, 95%CI 1.62-4.52). This study highlights the need for adapted adherence support and service delivery models for both adolescents and young adults.
Conflict of interest statement
Figures
Similar articles
-
Adolescents living with HIV are at higher risk of death and loss to follow up from care: Analysis of cohort data from eight health facilities in Ethiopia.PLoS One. 2019 Oct 17;14(10):e0223655. doi: 10.1371/journal.pone.0223655. eCollection 2019. PLoS One. 2019. PMID: 31622391 Free PMC article.
-
Modelling adverse treatment outcomes of HIV-infected adolescents attending public-sector HIV clinics in Lusaka.Public Health. 2017 Jun;147:8-14. doi: 10.1016/j.puhe.2017.01.022. Epub 2017 Mar 6. Public Health. 2017. PMID: 28404502
-
Treatment outcomes of HIV-infected adolescents attending public-sector HIV clinics across Gauteng and Mpumalanga, South Africa.AIDS Res Hum Retroviruses. 2013 Jun;29(6):892-900. doi: 10.1089/AID.2012.0215. Epub 2013 Feb 25. AIDS Res Hum Retroviruses. 2013. PMID: 23373540 Free PMC article.
-
Relationship Between Time to Initiation of Antiretroviral Therapy and Treatment Outcomes: A Cohort Analysis of ART Eligible Adolescents in Zimbabwe.J Acquir Immune Defic Syndr. 2017 Apr 1;74(4):390-398. doi: 10.1097/QAI.0000000000001274. J Acquir Immune Defic Syndr. 2017. PMID: 28002183 Free PMC article.
-
Treatment outcomes in HIV-infected adolescents attending a community-based antiretroviral therapy clinic in South Africa.BMC Infect Dis. 2012 Jan 25;12:21. doi: 10.1186/1471-2334-12-21. BMC Infect Dis. 2012. PMID: 22273267 Free PMC article.
Cited by
-
Effectiveness of community adolescent treatment supporters (CATS) interventions in improving linkage and retention in care, adherence to ART and psychosocial well-being: a randomised trial among adolescents living with HIV in rural Zimbabwe.BMC Public Health. 2019 Jan 28;19(1):117. doi: 10.1186/s12889-019-6447-4. BMC Public Health. 2019. PMID: 30691425 Free PMC article. Clinical Trial.
-
Incidence and Progression of Echocardiographic Abnormalities in Older Children with Human Immunodeficiency Virus and Adolescents Taking Antiretroviral Therapy: A Prospective Cohort Study.Clin Infect Dis. 2020 Mar 17;70(7):1372-1378. doi: 10.1093/cid/ciz373. Clin Infect Dis. 2020. PMID: 31054255 Free PMC article.
-
Getting to 90-90-90 targets for children and adolescents HIV in low and concentrated epidemics: bottlenecks, opportunities, and solutions.Curr Opin HIV AIDS. 2016 Mar;11 Suppl 1(Suppl 1):S1-5. doi: 10.1097/COH.0000000000000264. Curr Opin HIV AIDS. 2016. PMID: 26945141 Free PMC article. Review. No abstract available.
-
Contemporary issues on the epidemiology and antiretroviral adherence of HIV-infected adolescents in sub-Saharan Africa: a narrative review.J Int AIDS Soc. 2015 Sep 16;18(1):20049. doi: 10.7448/IAS.18.1.20049. eCollection 2015. J Int AIDS Soc. 2015. PMID: 26385853 Free PMC article. Review.
-
Tuberculosis infection and disease in South African adolescents with perinatally acquired HIV on antiretroviral therapy: a cohort study.J Int AIDS Soc. 2021 Mar;24(3):e25671. doi: 10.1002/jia2.25671. J Int AIDS Soc. 2021. PMID: 33719199 Free PMC article.
References
-
- Anon (2011) Opportunity in crisis. Preventing HIV from adolescence to young adulthood. UNICEF, UNAIDS, UNESCO, UNFPA, ILO, WHO and The World Bank: New York.
-
- Anon (2010) UNAIDS Report on the Global AIDS Epidemic. UNAIDS: Geneva.
-
- Flynn PM, Rudy BJ, Lindsey JC, Douglas SD, Lathey J, et al. (2007) Long-term observation of adolescents initiating HAART therapy: three-year follow-up. AIDS Res Hum Retroviruses 23: 1208–14. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
