

Ability of procalcitonin to discriminate infection from non-infective inflammation using two pleural disease settings
- PMID: 23251353
- PMCID: PMC3520973
- DOI: 10.1371/journal.pone.0049894
Ability of procalcitonin to discriminate infection from non-infective inflammation using two pleural disease settings
Abstract
Procalcitonin has been shown to be useful in separating infection from non-infective disorders. However, infection is often paralleled by tissue inflammation. Most studies supporting the use of procalcitonin were confounded by more significant inflammation in the infection group. Few studies have examined the usefulness of procalcitonin when adjusted for inflammation.Pleural inflammation underlies the development of most exudative effusions including pleural infection and malignancy. Pleurodesis, often used to treat effusions, involves provocation of intense aseptic pleural inflammation. We conducted a two-part proof-of-concept study to test the specificity of procalcitonin in differentiating infection using cohorts of patients with pleural effusions of infective and non-infective etiologies, as well as subjects undergoing pleurodesis.
Methods: We measured the blood procalcitonin level (i) in 248 patients with pleural infection or with non-infective pleural inflammation, matched for severity of systemic inflammation by C-reactive protein (CRP), age and gender; and (ii) in patients before and 24-48 hours after induction of non-infective pleural inflammation (from talc pleurodesis).
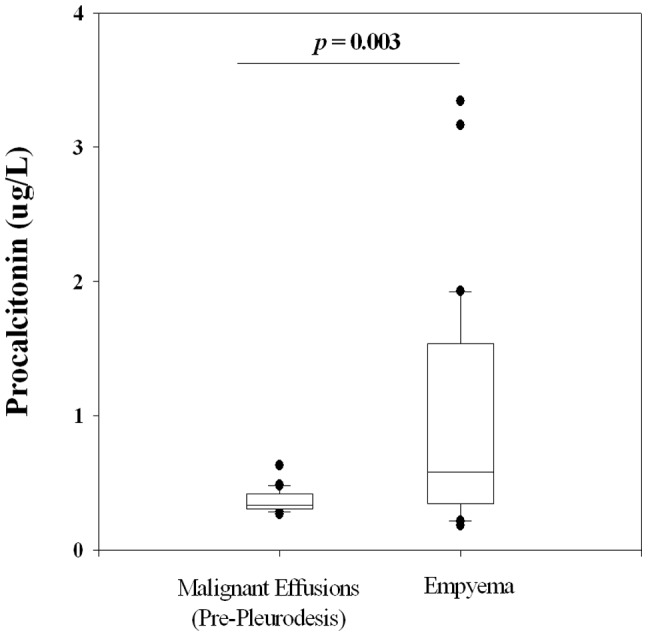
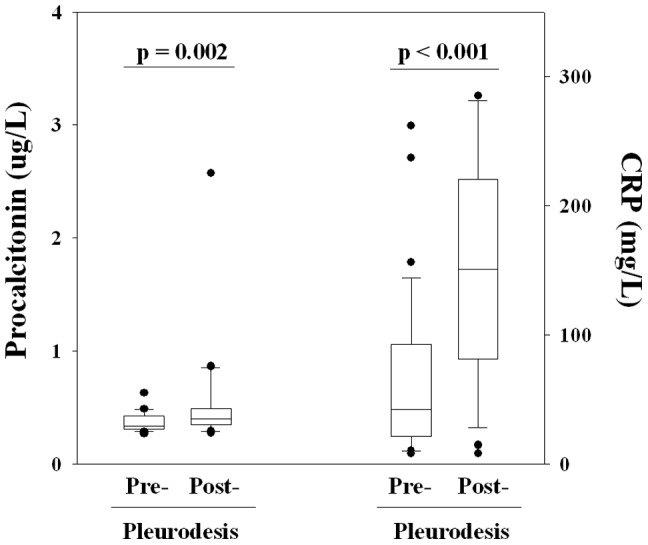
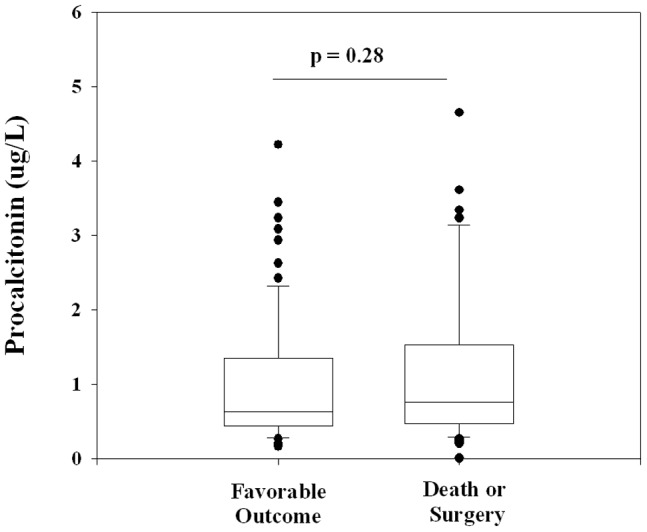
Results: 1) Procalcitonin was significantly higher in patients with pleural infection compared with controls with non-infective effusions (n = 32 each group) that were case-matched for systemic inflammation as measured by CRP [median (25-75%IQR): 0.58 (0.35-1.50) vs 0.34 (0.31-0.42) µg/L respectively, p = 0.003]. 2) Talc pleurodesis provoked intense systemic inflammation, and raised serum CRP by 360% over baseline. However procalcitonin remained relatively unaffected (21% rise). 3) Procalcitonin and CRP levels did not correlate. In 214 patients with pleural infection, procalcitonin levels did not predict the survival or need for surgical intervention.
Conclusion: Using a pleural model, this proof-of-principle study confirmed that procalcitonin is a biomarker specific for infection and is not affected by non-infective inflammation. Procalcitonin is superior to CRP in distinguishing infection from non-infective pleural diseases, even when controlled for the level of systemic inflammation.
Conflict of interest statement
Figures
Similar articles
-
The role of serum procalcitonin in establishing the diagnosis and prognosis of pleural infection.Respir Res. 2017 Feb 3;18(1):30. doi: 10.1186/s12931-017-0501-5. Respir Res. 2017. PMID: 28158976 Free PMC article. Clinical Trial.
-
Differential diagnosis of bacterial infection and inflammatory response in kidney diseases using procalcitonin.J Nephrol. 2002 May-Jun;15(3):297-301. J Nephrol. 2002. PMID: 12113602
-
Procalcitonin in patients with acute and chronic renal insufficiency.Wien Klin Wochenschr. 2004 Dec 30;116(24):849-53. doi: 10.1007/s00508-004-0279-6. Wien Klin Wochenschr. 2004. PMID: 15690970
-
Diagnostic accuracies of procalcitonin and C-reactive protein for bacterial infection in patients with systemic rheumatic diseases: a meta-analysis.Clin Exp Rheumatol. 2015 Mar-Apr;33(2):166-73. Epub 2015 Jan 20. Clin Exp Rheumatol. 2015. PMID: 25602442 Review.
-
Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections.Evid Based Child Health. 2013 Jul;8(4):1297-371. doi: 10.1002/ebch.1927. Evid Based Child Health. 2013. PMID: 23877944 Review.
Cited by
-
Recent Insights into the Management of Pleural Infection.Int J Gen Med. 2021 Jul 14;14:3415-3429. doi: 10.2147/IJGM.S292705. eCollection 2021. Int J Gen Med. 2021. PMID: 34290522 Free PMC article. Review.
-
Can Procalcitonin in Cerebrospinal Fluid be a Diagnostic Tool for Meningitis?J Clin Lab Anal. 2015 May;29(3):169-74. doi: 10.1002/jcla.21746. Epub 2014 May 5. J Clin Lab Anal. 2015. PMID: 24797775 Free PMC article.
-
Diagnostic Accuracy of Procalcitonin, Neutrophil-to-Lymphocyte Ratio, and C-Reactive Protein in Detection of Bacterial Infections and Prediction of Outcome in Nonneutropenic Febrile Patients with Lung Malignancy.J Oncol. 2020 Aug 25;2020:2192378. doi: 10.1155/2020/2192378. eCollection 2020. J Oncol. 2020. PMID: 32908505 Free PMC article.
-
Chronic empyema: importance of preventing complications in the management of pleural effusions.BMJ Case Rep. 2013 Aug 14;2013:bcr2013200454. doi: 10.1136/bcr-2013-200454. BMJ Case Rep. 2013. PMID: 23946529 Free PMC article.
-
Diagnostic Accuracy of Procalcitonin in Bacterial Meningitis Versus Nonbacterial Meningitis: A Systematic Review and Meta-Analysis.Medicine (Baltimore). 2016 Mar;95(11):e3079. doi: 10.1097/MD.0000000000003079. Medicine (Baltimore). 2016. PMID: 26986140 Free PMC article. Review.
References
-
- Schuetz P, Amin DN, Greenwald JL (2012) Role of procalcitonin in managing adult patients with respiratory tract infections. Chest 141: 1063–73. - PubMed
-
- Becker KL, Snider R, Nylen ES (2008) Procalcitonin assay in systemic inflammation, infection, and sepsis: clinical utility and limitations. Crit Care Med 36: 941–52. - PubMed
-
- Russwurm S, Wiederhold M, Oberhoffer M, Stonans I, Zipfel PF, et al. (1999) Molecular aspects and natural source of procalcitonin. Clin Chem Lab Med 37: 789–97. - PubMed
-
- Olah A, Belágyi T, Issekutz A, Makay R, Zaborszky A (2005) Value of procalcitonin quick test in the differentiation between sterile and infected forms of acute pancreatitis. Hepatogastroenterology 52: 243–5. - PubMed
-
- Brunkhorst FM, Eberhard OK, Brunkhorst R (1999) Discrimination of infectious and noninfectious causes of early acute respiratory distress syndrome by procalcitonin. Crit Care Med 27: 2172–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
