

Mortality from ischaemic heart disease by country, region, and age: statistics from World Health Organisation and United Nations
- PMID: 23218570
- PMCID: PMC3819990
- DOI: 10.1016/j.ijcard.2012.10.046
Mortality from ischaemic heart disease by country, region, and age: statistics from World Health Organisation and United Nations
Abstract
Background: Ischaemic heart disease (IHD) is the leading cause of death worldwide. The World Health Organisation (WHO) collects mortality data coded using the International Statistical Classification of Diseases (ICD) code.
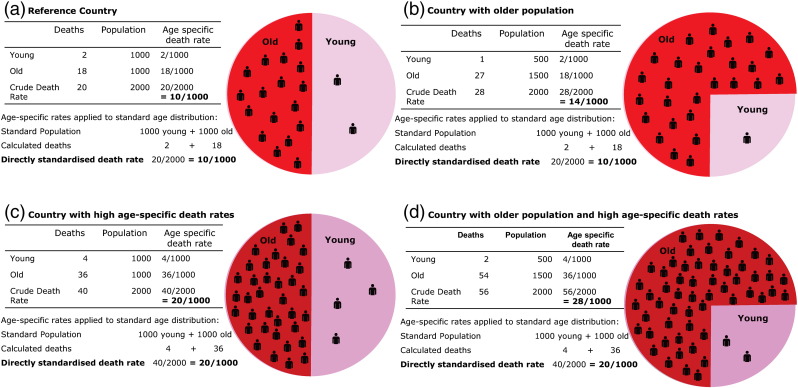
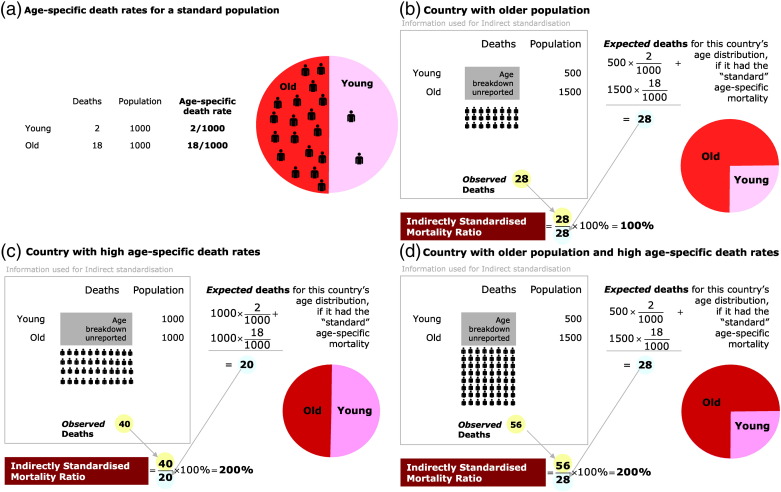
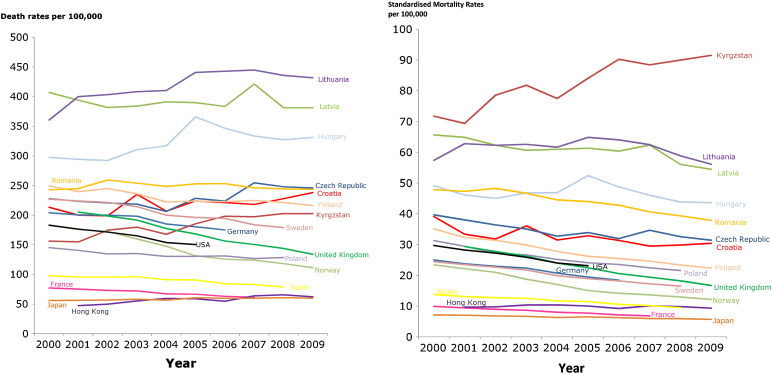
Methods: We analysed IHD deaths world-wide between 1995 and 2009 and used the UN population database to calculate age-specific and directly and indirectly age-standardised IHD mortality rates by country and region.
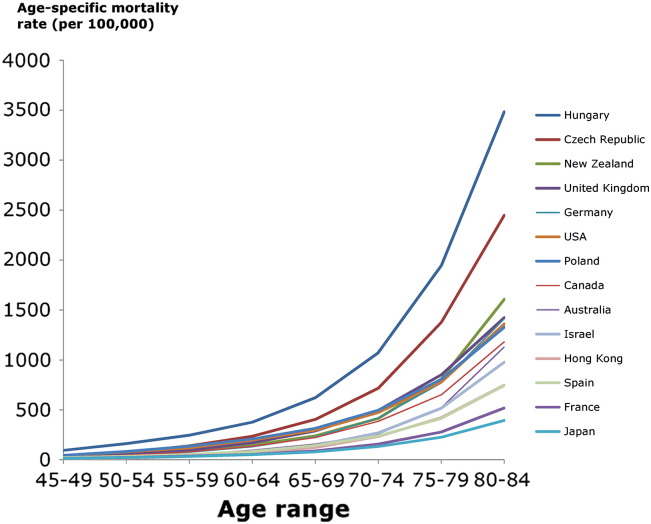
Results: IHD is the single largest cause of death worldwide, causing 7,249,000 deaths in 2008, 12.7% of total global mortality. There is more than 20-fold variation in IHD mortality rates between countries. Highest IHD mortality rates are in Eastern Europe and Central Asian countries; lowest rates in high income countries. For the working-age population, IHD mortality rates are markedly higher in low-and-middle income countries than in high income countries. Over the last 25 years, age-standardised IHD mortality has fallen by more than half in high income countries, but the trend is flat or increasing in some low-and-middle income countries. Low-and-middle income countries now account for more than 80% of global IHD deaths.
Conclusions: The global burden of IHD deaths has shifted to low-and-middle income countries as lifestyles approach those of high income countries. In high income countries, population ageing maintains IHD as the leading cause of death. Nevertheless, the progressive decline in age-standardised IHD mortality in high income countries shows that increasing IHD mortality is not inevitable. The 20-fold mortality difference between countries, and the temporal trends, may hold vital clues for handling IHD epidemic which is migratory, and still burgeoning.
Keywords: Coronary heart disease; Ischaemic heart disease; Mortality; Trends.
Copyright © 2012 Elsevier Ireland Ltd. All rights reserved.
Figures
Similar articles
-
2014 global geographic analysis of mortality from ischaemic heart disease by country, age and income: statistics from World Health Organisation and United Nations.Int J Cardiol. 2014 Jun 15;174(2):293-8. doi: 10.1016/j.ijcard.2014.04.096. Epub 2014 Apr 13. Int J Cardiol. 2014. PMID: 24794549 Free PMC article.
-
Temporal trends in ischemic heart disease mortality in 21 world regions, 1980 to 2010: the Global Burden of Disease 2010 study.Circulation. 2014 Apr 8;129(14):1483-92. doi: 10.1161/CIRCULATIONAHA.113.004042. Epub 2014 Feb 26. Circulation. 2014. PMID: 24573352 Free PMC article. Review.
-
Mortality From Ischemic Heart Disease.Circ Cardiovasc Qual Outcomes. 2019 Jun;12(6):e005375. doi: 10.1161/CIRCOUTCOMES.118.005375. Epub 2019 Jun 4. Circ Cardiovasc Qual Outcomes. 2019. PMID: 31163980 Free PMC article.
-
Variations in ischemic heart disease burden by age, country, and income: the Global Burden of Diseases, Injuries, and Risk Factors 2010 study.Glob Heart. 2014 Mar;9(1):91-9. doi: 10.1016/j.gheart.2013.12.007. Glob Heart. 2014. PMID: 24977114 Free PMC article.
-
The changing face of cardiovascular disease 2000-2012: An analysis of the world health organisation global health estimates data.Int J Cardiol. 2016 Dec 1;224:256-264. doi: 10.1016/j.ijcard.2016.09.026. Epub 2016 Sep 15. Int J Cardiol. 2016. PMID: 27664572 Review.
Cited by
-
Uncovering the Mechanism of Chinese Hawthorn Leaf on Myocardial Ischemia Based on Network Pharmacology, Molecular Docking Verification, and In Vitro Studies.Cardiovasc Toxicol. 2024 Feb;24(2):171-183. doi: 10.1007/s12012-024-09825-w. Epub 2024 Feb 20. Cardiovasc Toxicol. 2024. PMID: 38376772
-
Dab2 gene variant is associated with increased coronary artery disease risk in Chinese Han population.Medicine (Baltimore). 2020 Jul 2;99(27):e20924. doi: 10.1097/MD.0000000000020924. Medicine (Baltimore). 2020. PMID: 32629690 Free PMC article.
-
Tissue-Based Predictors of Impaired Right Ventricular Strain in Coronary Artery Disease: A Multicenter Stress Perfusion Study.Circ Cardiovasc Imaging. 2024 Aug;17(8):e016852. doi: 10.1161/CIRCIMAGING.124.016852. Epub 2024 Aug 20. Circ Cardiovasc Imaging. 2024. PMID: 39163376
-
Burden of non-communicable diseases in Iraq after the 2003 war.Saudi Med J. 2019 Jan;40(1):72-78. doi: 10.15537/smj.2019.1.23463. Saudi Med J. 2019. PMID: 30617384 Free PMC article.
-
Patterns of Medicare-funded primary health and specialist consultations in Aboriginal and non-Aboriginal Australians in the two years before hospitalisation for ischaemic heart disease.Int J Equity Health. 2018 Aug 2;17(1):111. doi: 10.1186/s12939-018-0826-9. Int J Equity Health. 2018. PMID: 30068346 Free PMC article.
References
-
- Xu J.Q., Kochanek K.D., Murphy S.L., Tejada-Vera B. vol. 58 no. 19. National Center for Health Statistics; Hyattsville, MD: 2010. Deaths: final data for 2007. (National vital statistics reports). - PubMed
-
- Scarborough P., Wickramasinghe K., Bhatnagar P., Rayner M. British Heart Foundation; London: 2011. Trends in coronary heart disease 1961–2011.
-
- Rosamond W., Flegal K., Furie K. Heart disease and stroke statistics—2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117(4):e25–e146. - PubMed
-
- Scarborough P., Bhatnagar P., Wickramasinghe K., Smolina K., Mitchell C., Rayner M. British Heart Foundation; 2010. Coronary heart disease statistics.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
