

Molecular pathogenesis of pulmonary arterial hypertension
- PMID: 23202738
- PMCID: PMC3533531
- DOI: 10.1172/JCI60658
Molecular pathogenesis of pulmonary arterial hypertension
Abstract
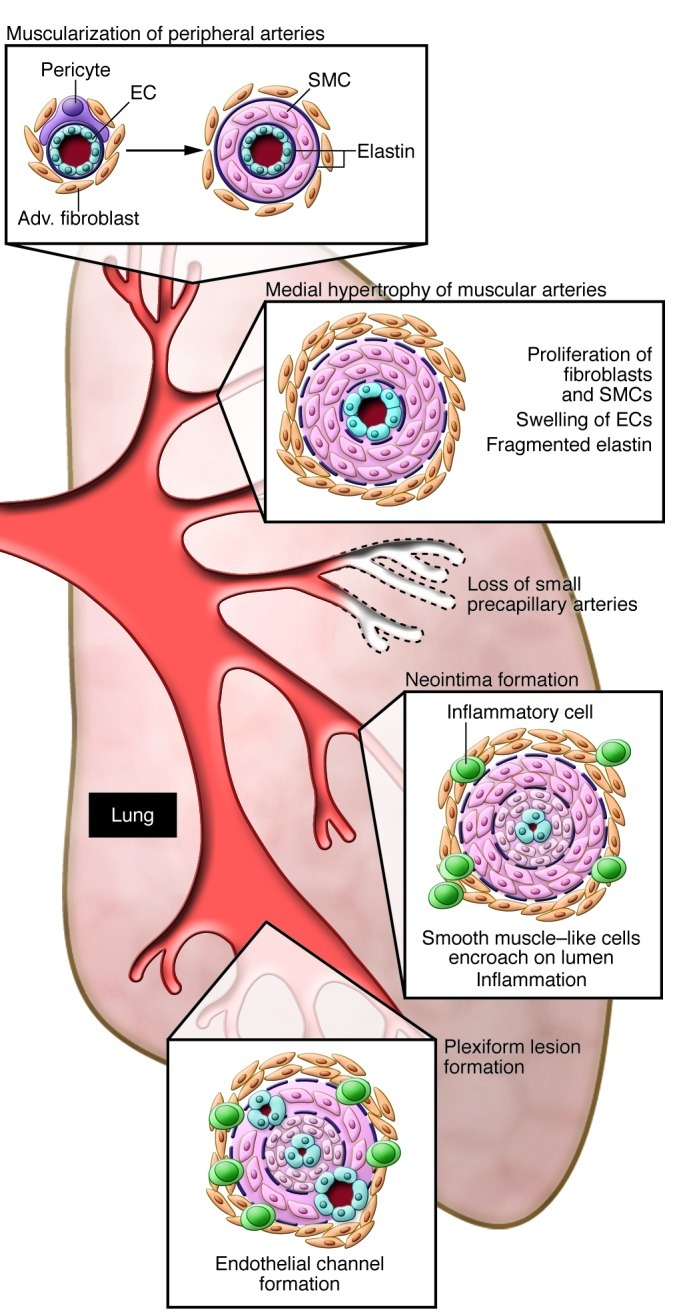
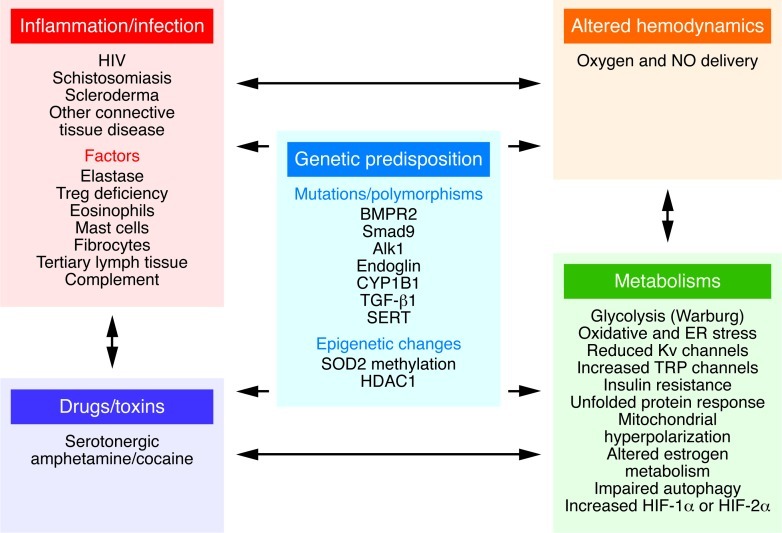
Recent clinical and experimental studies are redefining the cellular and molecular bases of pulmonary arterial hypertension (PAH). The genetic abnormalities first identified in association with the idiopathic form of PAH--together with a vast increase in our understanding of cell signaling, cell transformation, and cell-cell interactions; gene expression; microRNA processing; and mitochondrial and ion channel function--have helped explain the abnormal response of vascular cells to injury. Experimental and clinical studies now converge on the intersection and interactions between a genetic predisposition involving the BMPR2 signaling pathway and an impaired metabolic and chronic inflammatory state in the vessel wall. These deranged processes culminate in an exuberant proliferative response that occludes the pulmonary arterial (PA) lumen and obliterates the most distal intraacinar vessels. Here, we describe emerging therapies based on preclinical studies that address these converging pathways.
Figures
Similar articles
-
Codependence of Bone Morphogenetic Protein Receptor 2 and Transforming Growth Factor-β in Elastic Fiber Assembly and Its Perturbation in Pulmonary Arterial Hypertension.Arterioscler Thromb Vasc Biol. 2017 Aug;37(8):1559-1569. doi: 10.1161/ATVBAHA.117.309696. Epub 2017 Jun 15. Arterioscler Thromb Vasc Biol. 2017. PMID: 28619995 Free PMC article.
-
Bmpr2 Mutant Rats Develop Pulmonary and Cardiac Characteristics of Pulmonary Arterial Hypertension.Circulation. 2019 Feb 12;139(7):932-948. doi: 10.1161/CIRCULATIONAHA.118.033744. Circulation. 2019. PMID: 30586714
-
Serotonin increases susceptibility to pulmonary hypertension in BMPR2-deficient mice.Circ Res. 2006 Mar 31;98(6):818-27. doi: 10.1161/01.RES.0000215809.47923.fd. Epub 2006 Feb 23. Circ Res. 2006. PMID: 16497988
-
Sex Differences in Pulmonary Hypertension.Clin Chest Med. 2021 Mar;42(1):217-228. doi: 10.1016/j.ccm.2020.10.005. Epub 2021 Jan 13. Clin Chest Med. 2021. PMID: 33541615 Review.
-
BMP type II receptor as a therapeutic target in pulmonary arterial hypertension.Cell Mol Life Sci. 2017 Aug;74(16):2979-2995. doi: 10.1007/s00018-017-2510-4. Epub 2017 Apr 26. Cell Mol Life Sci. 2017. PMID: 28447104 Free PMC article. Review.
Cited by
-
Prostacyclin Analogues Inhibit Platelet Reactivity, Extracellular Vesicle Release and Thrombus Formation in Patients with Pulmonary Arterial Hypertension.J Clin Med. 2021 Mar 2;10(5):1024. doi: 10.3390/jcm10051024. J Clin Med. 2021. PMID: 33801460 Free PMC article.
-
Targeted therapies for systemic sclerosis.Nat Rev Rheumatol. 2013 Aug;9(8):451-64. doi: 10.1038/nrrheum.2013.46. Epub 2013 Apr 9. Nat Rev Rheumatol. 2013. PMID: 23567456 Review.
-
Cathepsin S Inhibition Suppresses Experimental Systemic Lupus Erythematosus-Associated Pulmonary Arterial Remodeling.Int J Mol Sci. 2022 Oct 14;23(20):12316. doi: 10.3390/ijms232012316. Int J Mol Sci. 2022. PMID: 36293172 Free PMC article.
-
New guidelines for managing pulmonary hypertension: what the pediatrician needs to know.Curr Opin Pediatr. 2016 Oct;28(5):597-606. doi: 10.1097/MOP.0000000000000403. Curr Opin Pediatr. 2016. PMID: 27583409 Free PMC article. Review.
-
Executive Summary of the American Heart Association and American Thoracic Society Joint Guidelines for Pediatric Pulmonary Hypertension.Am J Respir Crit Care Med. 2016 Oct 1;194(7):898-906. doi: 10.1164/rccm.201606-1183ST. Am J Respir Crit Care Med. 2016. PMID: 27689707 Free PMC article.
References
-
- Rabinovitch M, et al. Pulmonary artery endothelial abnormalities in patients with congenital heart defects and pulmonary hypertension: A correlation of light with scanning electron microscopy and transmission electron microscopy. Lab Invest. 1986;55(6):632–653. - PubMed
-
- Rosenberg HC, Rabinovitch M. Endothelial injury and vascular reactivity in monocrotaline pulmonary hypertension. Am J Physiol. 1988;255(6 pt 2):H1484–H1491. - PubMed
-
- Thompson K, Rabinovitch M. Exogenous leukocyte and endogenous elastases can mediate mitogenic activity in pulmonary artery smooth muscle cells by release of extracellular-matrix bound basic fibroblast growth factor. J Cell Physiol. 1996;166(3):495–505. doi: 10.1002/(SICI)1097-4652(199603)166:3<495::AID-JCP4>3.0.CO;2-K. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
