

Myocardial recovery and the failing heart: myth, magic, or molecular target?
- PMID: 23158527
- PMCID: PMC3522780
- DOI: 10.1016/j.jacc.2012.06.062
Myocardial recovery and the failing heart: myth, magic, or molecular target?
Abstract
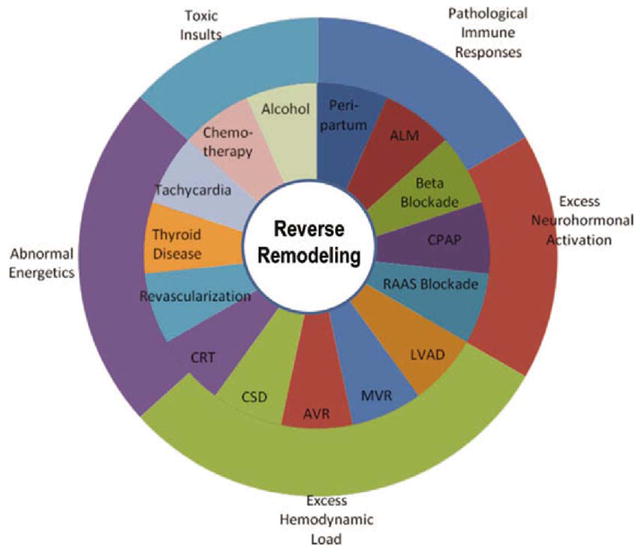
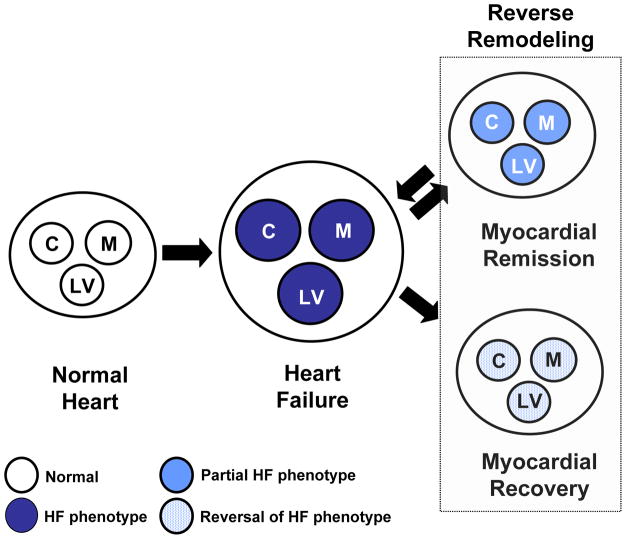
Medical and device therapies that reduce heart failure morbidity and mortality also lead to decreased left ventricular volume and mass and a more normal elliptical shape of the ventricle. These are due to changes in myocyte size, structure, and organization that have been referred to collectively as reverse remodeling. Moreover, there are subsets of patients whose hearts have undergone reverse remodeling either spontaneously or after medical or device therapies and whose clinical course is associated with freedom from future heart failure events. This phenomenon has been referred to as myocardial recovery. Despite the frequent interchangeable use of the terms "myocardial recovery" and "reverse remodeling" to describe the reversal of various aspects of the heart failure phenotype after medical and device therapy, the literature suggests that there are important differences between these 2 phenomena and that myocardial recovery and reverse remodeling are not synonymous. In this review, we discuss the biology of cardiac remodeling, cardiac reverse remodeling, and myocardial recovery with the intent to provide a conceptual framework for understanding myocardial recovery.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures

Similar articles
-
Is myocardial recovery possible and how do you measure it?Curr Cardiol Rep. 2012 Jun;14(3):293-8. doi: 10.1007/s11886-012-0264-z. Curr Cardiol Rep. 2012. PMID: 22437373 Review.
-
Myocardial recovery and the failing heart: medical, device and mechanical methods.Ann Glob Health. 2014 Jan-Feb;80(1):55-60. doi: 10.1016/j.aogh.2013.12.006. Epub 2013 Dec 25. Ann Glob Health. 2014. PMID: 24751565 Review.
-
Comparison of left ventricular reverse remodeling induced by cardiac contractility modulation and cardiac resynchronization therapy in heart failure patients with different QRS durations.Int J Cardiol. 2013 Aug 10;167(3):889-93. doi: 10.1016/j.ijcard.2012.01.066. Epub 2012 Feb 12. Int J Cardiol. 2013. PMID: 22330007
-
Reverse remodelling and myocardial recovery in heart failure.Nat Rev Cardiol. 2018 Feb;15(2):83-96. doi: 10.1038/nrcardio.2017.139. Epub 2017 Sep 21. Nat Rev Cardiol. 2018. PMID: 28933783 Review.
-
Changing the remodeling process in heart failure: basic mechanisms and laboratory results.Curr Opin Cardiol. 1998 May;13(3):156-61. Curr Opin Cardiol. 1998. PMID: 9649937 Review.
Cited by
-
Association of early versus delayed normalisation of left ventricular ejection fraction with mortality in ischemic cardiomyopathy.Open Heart. 2021 Mar;8(1):e001528. doi: 10.1136/openhrt-2020-001528. Open Heart. 2021. PMID: 33723015 Free PMC article. Clinical Trial.
-
Myocardial Recovery in Cardiogenic Shock.Methodist Debakey Cardiovasc J. 2024 Aug 20;20(4):64-75. doi: 10.14797/mdcvj.1383. eCollection 2024. Methodist Debakey Cardiovasc J. 2024. PMID: 39184158 Free PMC article. Review.
-
Neurohormonal activation in heart failure with reduced ejection fraction.Nat Rev Cardiol. 2017 Jan;14(1):30-38. doi: 10.1038/nrcardio.2016.163. Epub 2016 Oct 6. Nat Rev Cardiol. 2017. PMID: 27708278 Free PMC article. Review.
-
Predictors of non-response to cardiac resynchronization therapy implantation in patients with class I indications: the markedly dilated left ventricular end-diastolic dimension and the presence of fragmented QRS.J Geriatr Cardiol. 2019 Jul;16(7):514-521. doi: 10.11909/j.issn.1671-5411.2019.07.009. J Geriatr Cardiol. 2019. PMID: 31447890 Free PMC article.
-
Heart failure with mid-range ejection fraction: pro and cons of the new classification of Heart Failure by European Society of Cardiology guidelines.ESC Heart Fail. 2020 Apr;7(2):381-399. doi: 10.1002/ehf2.12586. Epub 2020 Apr 1. ESC Heart Fail. 2020. PMID: 32239646 Free PMC article. Review.
References
-
- Kass DA, Baughman KL, Pak PH, et al. Reverse remodeling from cardiomyoplasty in human heart failure. External constraint versus active assist. Circulation. 1995;91:2314–8. - PubMed
-
- Levin HR, Oz MC, Chen JM, Packer M, Rose EA, Burkhoff D. Reversal of chronic ventricular dilation in patients with end-stage cardiomyopathy by prolonged mechanical unloading. Circulation. 1995;91:2717–20. - PubMed
-
- Westaby S, Jin XY, Katsumata T, Taggart DP, Coats AJ, Frazier OH. Mechanical Support in Dilated Cardiomyopathy: Signs of Early Left Ventricular Recovery (abstr) Ann Thorac Surg. 1997;64:1303–1308. - PubMed
-
- Cohn JN, Ferrari R, Sharpe N. Cardiac remodeling--concepts and clinical implications: a consensus paper from an international forum on cardiac remodeling. Behalf of an International Forum on Cardiac Remodeling. J Am Coll Cardiol. 2000;35:569–82. - PubMed
-
- Mann DL. Mechanisms and models in heart failure: a combinatorial approach. Circulation. 1999;100:999–1088. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
