

Androgen receptor signaling in circulating tumor cells as a marker of hormonally responsive prostate cancer
- PMID: 23093251
- PMCID: PMC3508523
- DOI: 10.1158/2159-8290.CD-12-0222
Androgen receptor signaling in circulating tumor cells as a marker of hormonally responsive prostate cancer
Abstract
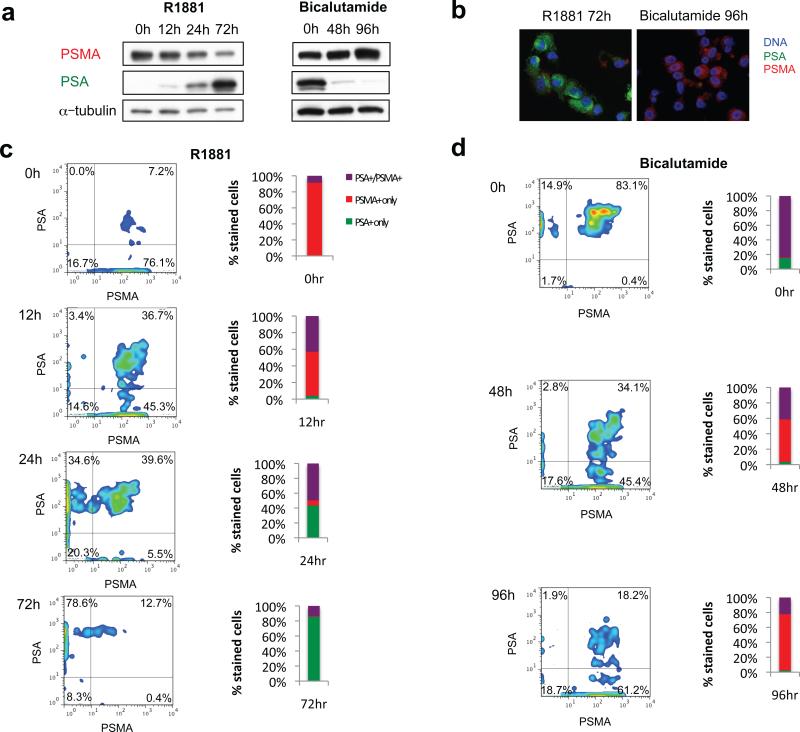
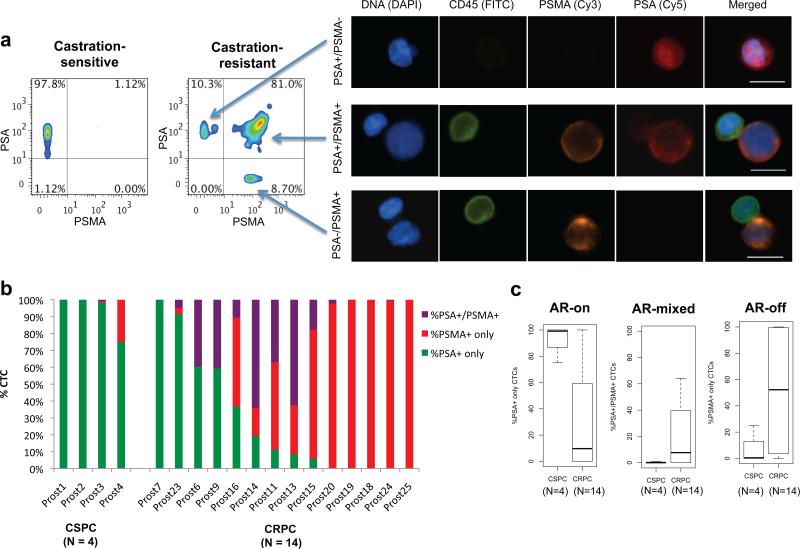
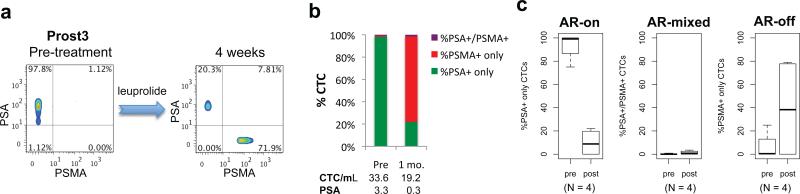
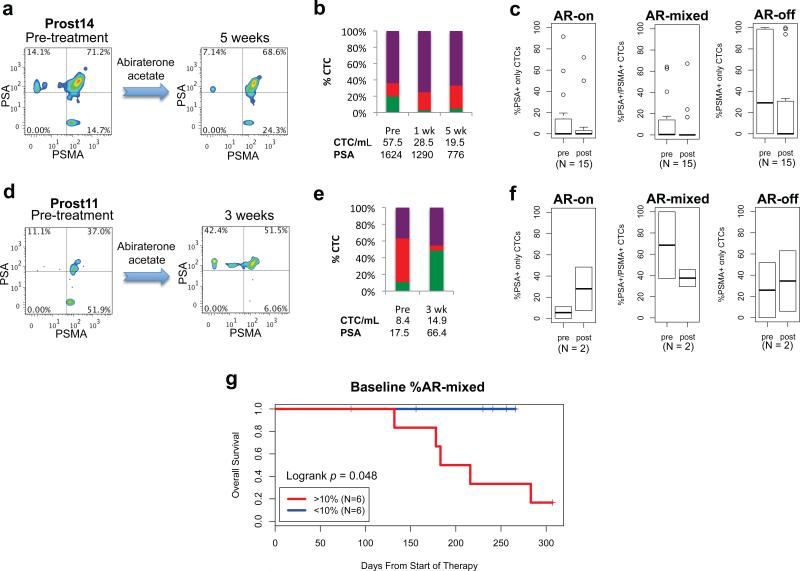
Androgen deprivation therapy (ADT) is initially effective in treating metastatic prostate cancer, and secondary hormonal therapies are being tested to suppress androgen receptor (AR) reactivation in castration-resistant prostate cancer (CRPC). Despite variable responses to AR pathway inhibitors in CRPC, there are no reliable biomarkers to guide their application. Here, we used microfluidic capture of circulating tumor cells (CTC) to measure AR signaling readouts before and after therapeutic interventions. Single-cell immunofluorescence analysis revealed predominantly "AR-on" CTC signatures in untreated patients, compared with heterogeneous ("AR-on, AR-off, and AR-mixed") CTC populations in patients with CRPC. Initiation of first-line ADT induced a profound switch from "AR-on" to "AR-off" CTCs, whereas secondary hormonal therapy in CRPC resulted in variable responses. Presence of "AR-mixed" CTCs and increasing "AR-on" cells despite treatment with abiraterone acetate were associated with an adverse treatment outcome. Measuring treatment-induced signaling responses within CTCs may help guide therapy in prostate cancer.
Significance: Acquired resistance to first-line hormonal therapy in prostate cancer is heterogeneous in the extent of AR pathway reactivation. Measurement of pre- and posttreatment AR signaling within CTCs may help target such treatments to patients most likely to respond to second-line therapies.
©2012 AACR.
Figures
Comment in
-
The potential of circulating tumor cells as a liquid biopsy to guide therapy in prostate cancer.Cancer Discov. 2012 Nov;2(11):974-5. doi: 10.1158/2159-8290.CD-12-0432. Epub 2012 Oct 23. Cancer Discov. 2012. PMID: 23093252
Similar articles
-
The potential of circulating tumor cells as a liquid biopsy to guide therapy in prostate cancer.Cancer Discov. 2012 Nov;2(11):974-5. doi: 10.1158/2159-8290.CD-12-0432. Epub 2012 Oct 23. Cancer Discov. 2012. PMID: 23093252
-
Distinct transcriptional programs mediated by the ligand-dependent full-length androgen receptor and its splice variants in castration-resistant prostate cancer.Cancer Res. 2012 Jul 15;72(14):3457-62. doi: 10.1158/0008-5472.CAN-11-3892. Epub 2012 Jun 18. Cancer Res. 2012. PMID: 22710436 Free PMC article.
-
Standardization of CTC AR-V7 PCR assay and evaluation of its role in castration resistant prostate cancer progression.Prostate. 2019 Jan;79(1):54-61. doi: 10.1002/pros.23710. Epub 2018 Aug 23. Prostate. 2019. PMID: 30141201
-
Androgen receptors in hormone-dependent and castration-resistant prostate cancer.Pharmacol Ther. 2013 Dec;140(3):223-38. doi: 10.1016/j.pharmthera.2013.07.003. Epub 2013 Jul 13. Pharmacol Ther. 2013. PMID: 23859952 Review.
-
Targeting the androgen receptor signaling pathway in advanced prostate cancer.Am J Health Syst Pharm. 2022 Jul 22;79(15):1224-1235. doi: 10.1093/ajhp/zxac105. Am J Health Syst Pharm. 2022. PMID: 35390118 Review.
Cited by
-
Lessons from tissue compartment-specific analysis of androgen receptor alterations in prostate cancer.J Steroid Biochem Mol Biol. 2017 Feb;166:28-37. doi: 10.1016/j.jsbmb.2016.04.016. Epub 2016 Apr 28. J Steroid Biochem Mol Biol. 2017. PMID: 27133384 Free PMC article. Review.
-
BMX controls 3βHSD1 and sex steroid biosynthesis in cancer.J Clin Invest. 2023 Jan 17;133(2):e163498. doi: 10.1172/JCI163498. J Clin Invest. 2023. PMID: 36647826 Free PMC article.
-
Characterization of a Prostate- and Prostate Cancer-Specific Circular RNA Encoded by the Androgen Receptor Gene.Mol Ther Nucleic Acids. 2019 Dec 6;18:916-926. doi: 10.1016/j.omtn.2019.10.015. Epub 2019 Oct 24. Mol Ther Nucleic Acids. 2019. PMID: 31760376 Free PMC article.
-
Capture and Detection of Circulating Glioma Cells Using the Recombinant VAR2CSA Malaria Protein.Cells. 2019 Aug 28;8(9):998. doi: 10.3390/cells8090998. Cells. 2019. PMID: 31466397 Free PMC article.
-
Genomic Analysis of Circulating Tumor Cells at the Single-Cell Level.J Mol Diagn. 2020 Jun;22(6):770-781. doi: 10.1016/j.jmoldx.2020.02.013. Epub 2020 Apr 2. J Mol Diagn. 2020. PMID: 32247862 Free PMC article.
References
-
- Scher HI, Sawyers CL. Biology of progressive, castration-resistant prostate cancer: directed therapies targeting the androgen-receptor signaling axis. J Clin Oncol. 2005;23:8253–61. - PubMed
-
- Chen CD, Welsbie DS, Tran C, Baek SH, Chen R, Vessella R, et al. Molecular determinants of resistance to antiandrogen therapy. Nat Med. 2004;10:33–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
