

Lung Injury Prevention with Aspirin (LIPS-A): a protocol for a multicentre randomised clinical trial in medical patients at high risk of acute lung injury
- PMID: 22952165
- PMCID: PMC3437429
- DOI: 10.1136/bmjopen-2012-001606
Lung Injury Prevention with Aspirin (LIPS-A): a protocol for a multicentre randomised clinical trial in medical patients at high risk of acute lung injury
Abstract
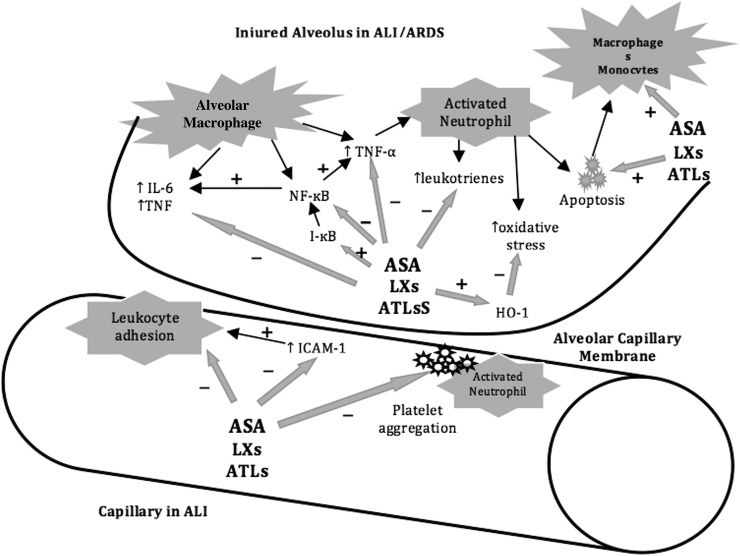
Introduction: Acute lung injury (ALI) is a devastating condition that places a heavy burden on public health resources. Although the need for effective ALI prevention strategies is increasingly recognised, no effective preventative strategies exist. The Lung Injury Prevention Study with Aspirin (LIPS-A) aims to test whether aspirin (ASA) could prevent and/or mitigate the development of ALI.
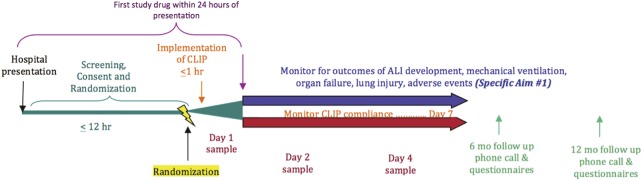
Methods and analysis: LIPS-A is a multicentre, double-blind, randomised clinical trial testing the hypothesis that the early administration of ASA will result in a reduced incidence of ALI in adult patients at high risk. This investigation will enrol 400 study participants from 14 hospitals across the USA. Conditional logistic regression will be used to test the primary hypothesis that early ASA administration will decrease the incidence of ALI.
Ethics and dissemination: Safety oversight will be under the direction of an independent Data and Safety Monitoring Board (DSMB). Approval of the protocol was obtained from the DSMB prior to enrolling the first study participant. Approval of both the protocol and informed consent documents were also obtained from the institutional review board of each participating institution prior to enrolling study participants at the respective site. In addition to providing important clinical and mechanistic information, this investigation will inform the scientific merit and feasibility of a phase III trial on ASA as an ALI prevention agent. The findings of this investigation, as well as associated ancillary studies, will be disseminated in the form of oral and abstract presentations at major national and international medical specialty meetings. The primary objective and other significant findings will also be presented in manuscript form. All final, published manuscripts resulting from this protocol will be submitted to Pub Med Central in accordance with the National Institute of Health Public Access Policy.
Figures
Similar articles
-
The Esophageal Pressure-Guided Ventilation 2 (EPVent2) trial protocol: a multicentre, randomised clinical trial of mechanical ventilation guided by transpulmonary pressure.BMJ Open. 2014 Oct 6;4(9):e006356. doi: 10.1136/bmjopen-2014-006356. BMJ Open. 2014. PMID: 25287106 Free PMC article. Clinical Trial.
-
Point-of-care washing of allogeneic red blood cells for the prevention of transfusion-related respiratory complications (WAR-PRC): a protocol for a multicenter randomised clinical trial in patients undergoing cardiac surgery.BMJ Open. 2017 Aug 18;7(8):e016398. doi: 10.1136/bmjopen-2017-016398. BMJ Open. 2017. PMID: 28821525 Free PMC article. Clinical Trial.
-
American Society of Clinical Oncology policy statement: oversight of clinical research.J Clin Oncol. 2003 Jun 15;21(12):2377-86. doi: 10.1200/JCO.2003.04.026. Epub 2003 Apr 29. J Clin Oncol. 2003. PMID: 12721281
-
Efaproxiral: GSJ 61, JP 4, KDD 86, RS 4, RSR 13.Drugs R D. 2005;6(3):178-85. doi: 10.2165/00126839-200506030-00007. Drugs R D. 2005. PMID: 15869322 Review.
-
Satraplatin: BMS 182751, BMY 45594, JM 216.Drugs R D. 2007;8(2):125-32. doi: 10.2165/00126839-200708020-00008. Drugs R D. 2007. PMID: 17324011 Review.
Cited by
-
Prehospital aspirin use is associated with reduced risk of acute respiratory distress syndrome in critically ill patients: a propensity-adjusted analysis.Crit Care Med. 2015 Apr;43(4):801-7. doi: 10.1097/CCM.0000000000000789. Crit Care Med. 2015. PMID: 25559436 Free PMC article.
-
Is there a need for emerging drugs for the acute respiratory distress syndrome?Expert Opin Emerg Drugs. 2014 Sep;19(3):323-8. doi: 10.1517/14728214.2014.953052. Epub 2014 Aug 24. Expert Opin Emerg Drugs. 2014. PMID: 25152048 Free PMC article.
-
Future therapies for ARDS.Intensive Care Med. 2015 Feb;41(2):322-6. doi: 10.1007/s00134-014-3578-z. Epub 2014 Dec 4. Intensive Care Med. 2015. PMID: 25472571 Free PMC article. No abstract available.
-
Prevention of acute respiratory distress syndrome.Curr Opin Crit Care. 2015 Feb;21(1):82-90. doi: 10.1097/MCC.0000000000000174. Curr Opin Crit Care. 2015. PMID: 25501020 Free PMC article. Review.
-
Platelets in the pathogenesis of acute respiratory distress syndrome.Am J Physiol Lung Cell Mol Physiol. 2015 Nov 1;309(9):L915-23. doi: 10.1152/ajplung.00266.2015. Epub 2015 Aug 28. Am J Physiol Lung Cell Mol Physiol. 2015. PMID: 26320157 Free PMC article. Review.
References
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute lung injury. N Engl J Med 2005;353:1685–93 - PubMed
-
- Herridge MS, Tansey CM, Matté A, et al. Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med 2011;364:1293–304 - PubMed
-
- Hudson LD, Milberg JA, Anardi D, et al. Clinical risks for development of the acute respiratory distress syndrome. Am J Respir Crit Care Med 1995;151:293–301 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources