

Delirium is a strong risk factor for dementia in the oldest-old: a population-based cohort study
- PMID: 22879644
- PMCID: PMC3437024
- DOI: 10.1093/brain/aws190
Delirium is a strong risk factor for dementia in the oldest-old: a population-based cohort study
Abstract
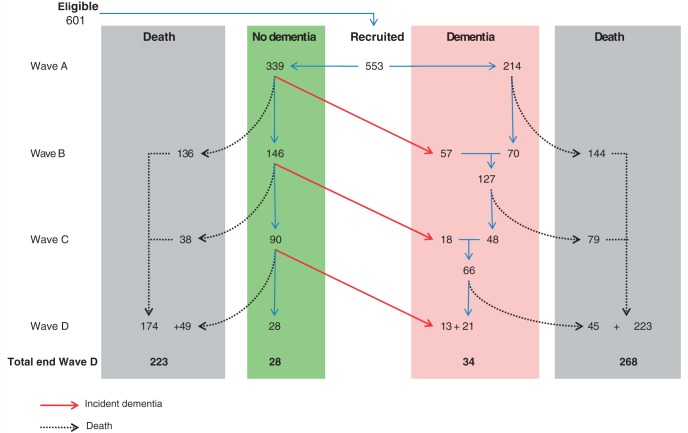
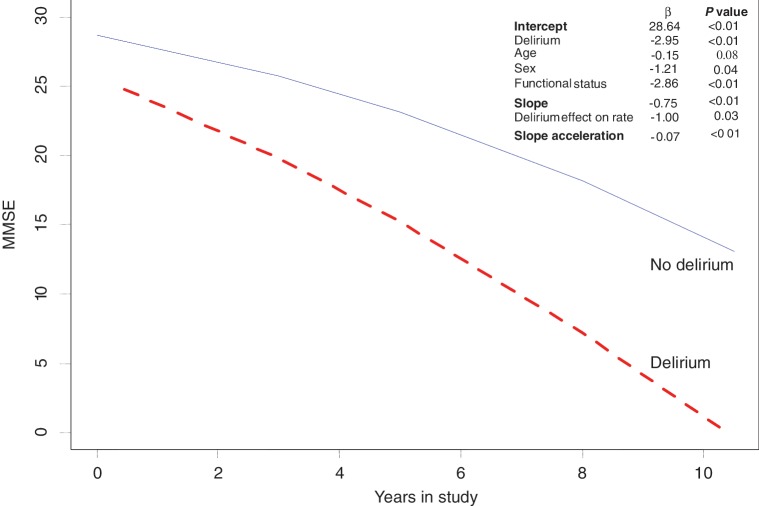
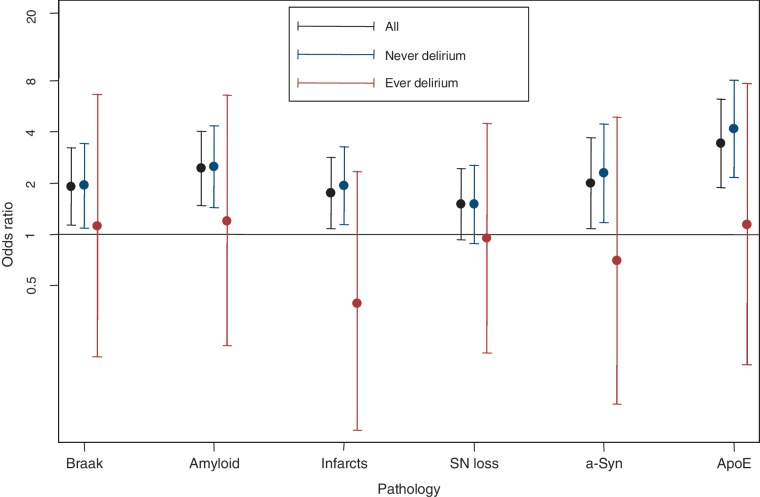
Recent studies suggest that delirium is associated with risk of dementia and also acceleration of decline in existing dementia. However, previous studies may have been confounded by incomplete ascertainment of cognitive status at baseline. Herein, we used a true population sample to determine if delirium is a risk factor for incident dementia and cognitive decline. We also examined the effect of delirium at the pathological level by determining associations between dementia and neuropathological markers of dementia in patients with and without a history of delirium. The Vantaa 85+ study examined 553 individuals (92% of those eligible) aged ≥85 years at baseline, 3, 5, 8 and 10 years. Brain autopsy was performed in 52%. Fixed and random-effects regression models were used to assess associations between (i) delirium and incident dementia and (ii) decline in Mini-Mental State Examination scores in the whole group. The relationship between dementia and common neuropathological markers (Alzheimer-type, infarcts and Lewy-body) was modelled, stratified by history of delirium. Delirium increased the risk of incident dementia (odds ratio 8.7, 95% confidence interval 2.1-35). Delirium was also associated with worsening dementia severity (odds ratio 3.1, 95% confidence interval 1.5-6.3) as well as deterioration in global function score (odds ratio 2.8, 95% confidence interval 1.4-5.5). In the whole study population, delirium was associated with loss of 1.0 more Mini-Mental State Examination points per year (95% confidence interval 0.11-1.89) than those with no history of delirium. In individuals with dementia and no history of delirium (n = 232), all pathologies were significantly associated with dementia. However, in individuals with delirium and dementia (n = 58), no relationship between dementia and these markers was found. For example, higher Braak stage was associated with dementia when no history of delirium (odds ratio 2.0, 95% confidence interval 1.1-3.5, P = 0.02), but in those with a history of delirium, there was no significant relationship (odds ratio 1.2, 95% confidence interval 0.2-6.7, P = 0.85). This trend for odds ratios to be closer to unity in the delirium and dementia group was observed for neuritic amyloid, apolipoprotein ε status, presence of infarcts, α-synucleinopathy and neuronal loss in substantia nigra. These findings are the first to demonstrate in a true population study that delirium is a strong risk factor for incident dementia and cognitive decline in the oldest-old. However, in this study, the relationship did not appear to be mediated by classical neuropathologies associated with dementia.
Figures
Comment in
-
Delirium, dementia and senility.Brain. 2012 Sep;135(Pt 9):2582-4. doi: 10.1093/brain/aws235. Brain. 2012. PMID: 22961542 No abstract available.
Similar articles
-
Delirium in older medical inpatients and subsequent cognitive and functional status: a prospective study.CMAJ. 2001 Sep 4;165(5):575-83. CMAJ. 2001. PMID: 11563209 Free PMC article.
-
Association of Delirium With Cognitive Decline in Late Life: A Neuropathologic Study of 3 Population-Based Cohort Studies.JAMA Psychiatry. 2017 Mar 1;74(3):244-251. doi: 10.1001/jamapsychiatry.2016.3423. JAMA Psychiatry. 2017. PMID: 28114436 Free PMC article.
-
Delirium, neurofilament light chain, and progressive cognitive impairment: analysis of a prospective Norwegian population-based cohort.Lancet Healthy Longev. 2023 Aug;4(8):e399-e408. doi: 10.1016/S2666-7568(23)00098-3. Epub 2023 Jul 14. Lancet Healthy Longev. 2023. PMID: 37459878
-
Dementia as a predictor of morbidity and mortality in patients with delirium.Maturitas. 2019 Jul;125:63-69. doi: 10.1016/j.maturitas.2019.03.005. Epub 2019 Apr 3. Maturitas. 2019. PMID: 31133220 Review.
-
Risk factors for incident delirium among older people in acute hospital medical units: a systematic review and meta-analysis.Age Ageing. 2014 May;43(3):326-33. doi: 10.1093/ageing/afu022. Epub 2014 Mar 6. Age Ageing. 2014. PMID: 24610863 Free PMC article. Review.
Cited by
-
New horizons in hospital-associated deconditioning: a global condition of body and mind.Age Ageing. 2024 Nov 1;53(11):afae241. doi: 10.1093/ageing/afae241. Age Ageing. 2024. PMID: 39497271 Free PMC article. Review.
-
Decoding the Neurological Sequelae of General Anesthesia: A Review.Med Sci Monit. 2024 Jan 23;30:e942740. doi: 10.12659/MSM.942740. Med Sci Monit. 2024. PMID: 38258288 Free PMC article. Review.
-
The incidence of mental disorder increases after hip fracture in older people: a nationwide cohort study.BMC Geriatr. 2021 Apr 15;21(1):249. doi: 10.1186/s12877-021-02195-w. BMC Geriatr. 2021. PMID: 33858356 Free PMC article.
-
Circadian Rest-Activity Rhythms, Delirium Risk, and Progression to Dementia.Ann Neurol. 2023 Jun;93(6):1145-1157. doi: 10.1002/ana.26617. Epub 2023 Mar 3. Ann Neurol. 2023. PMID: 36808743 Free PMC article.
-
Proteome-Wide Analysis Using SOMAscan Identifies and Validates Chitinase-3-Like Protein 1 as a Risk and Disease Marker of Delirium Among Older Adults Undergoing Major Elective Surgery.J Gerontol A Biol Sci Med Sci. 2022 Mar 3;77(3):484-493. doi: 10.1093/gerona/glaa326. J Gerontol A Biol Sci Med Sci. 2022. PMID: 35239952 Free PMC article.
References
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd edn. revised (DSM-III-R). Washington: American Psychiatric Association; 1987.
-
- Ahtiluoto S, Polvikoski T, Peltonen M, Solomon A, Tuomilehto J, Winblad B, et al. Diabetes, Alzheimer disease, and vascular dementia: a population-based neuropathologic study. Neurology. 2010;75:1195–202. - PubMed
-
- Brayne C, Ince PG, Keage HA, McKeith IG, Matthews FE, Polvikoski T, et al. Education, the brain and dementia: neuroprotection or compensation? Brain. 2010;133:2210–6. - PubMed
-
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
