

Concurrent expression of MYC and BCL2 in diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone
- PMID: 22851565
- PMCID: PMC3454768
- DOI: 10.1200/JCO.2011.41.0985
Concurrent expression of MYC and BCL2 in diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone
Abstract
Purpose: Diffuse large B-cell lymphoma (DLBCL) is curable in 60% of patients treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP). MYC translocations, with or without BCL2 translocations, have been associated with inferior survival in DLBCL. We investigated whether expression of MYC protein, with or without BCL2 protein expression, could risk-stratify patients at diagnosis.
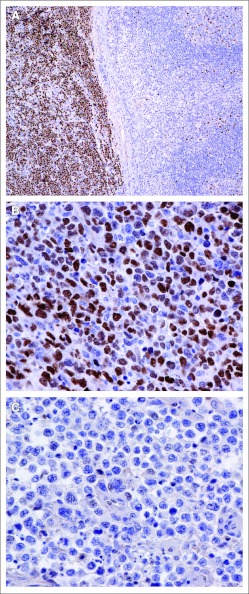
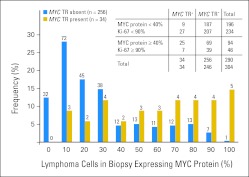
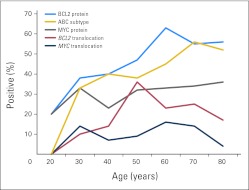
Patients and methods: We determined the correlation between presence of MYC and BCL2 proteins by immunohistochemistry (IHC) with survival in two independent cohorts of patients with DLBCL treated with R-CHOP. We further determined if MYC protein expression correlated with high MYC mRNA and/or presence of MYC translocation.
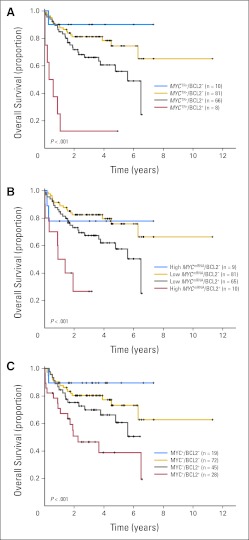
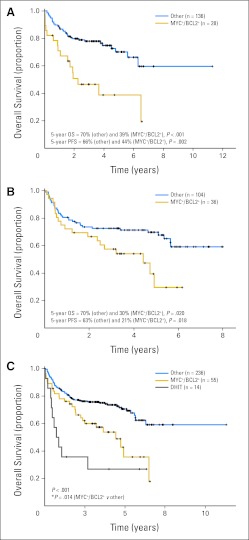
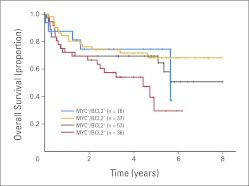
Results: In the training cohort (n = 167), MYC and BCL2 proteins were detected in 29% and 44% of patients, respectively. Concurrent expression (MYC positive/BCL2 positive) was present in 21% of patients. MYC protein correlated with presence of high MYC mRNA and MYC translocation (both P < .001), but the latter was less frequent (both 11%). MYC protein expression was only associated with inferior overall and progression-free survival when BCL2 protein was coexpressed (P < .001). Importantly, the poor prognostic effect of MYC positive/BCL2 positive was validated in an independent cohort of 140 patients with DLBCL and remained significant (P < .05) after adjusting for presence of high-risk features in a multivariable model that included elevated international prognostic index score, activated B-cell molecular subtype, and presence of concurrent MYC and BCL2 translocations.
Conclusion: Assessment of MYC and BCL2 expression by IHC represents a robust, rapid, and inexpensive approach to risk-stratify patients with DLBCL at diagnosis.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Growing importance of MYC/BCL2 immunohistochemistry in diffuse large B-cell lymphomas.J Clin Oncol. 2012 Oct 1;30(28):3433-5. doi: 10.1200/JCO.2012.44.4729. Epub 2012 Sep 4. J Clin Oncol. 2012. PMID: 22949148 No abstract available.
Similar articles
-
Immunohistochemical double-hit score is a strong predictor of outcome in patients with diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone.J Clin Oncol. 2012 Oct 1;30(28):3460-7. doi: 10.1200/JCO.2011.41.4342. Epub 2012 Jun 4. J Clin Oncol. 2012. PMID: 22665537
-
Patients with diffuse large B-cell lymphoma of germinal center origin with BCL2 translocations have poor outcome, irrespective of MYC status: a report from an International DLBCL rituximab-CHOP Consortium Program Study.Haematologica. 2013 Feb;98(2):255-63. doi: 10.3324/haematol.2012.066209. Epub 2012 Aug 28. Haematologica. 2013. PMID: 22929980 Free PMC article.
-
Clinical Impact of the Cell-of-Origin Classification and the MYC/ BCL2 Dual Expresser Status in Diffuse Large B-Cell Lymphoma Treated Within Prospective Clinical Trials of the German High-Grade Non-Hodgkin's Lymphoma Study Group.J Clin Oncol. 2017 Aug 1;35(22):2515-2526. doi: 10.1200/JCO.2016.70.3660. Epub 2017 May 19. J Clin Oncol. 2017. PMID: 28525305 Clinical Trial.
-
The Spectrum of MYC Alterations in Diffuse Large B-Cell Lymphoma.Acta Haematol. 2020;143(6):520-528. doi: 10.1159/000505892. Epub 2020 Feb 19. Acta Haematol. 2020. PMID: 32074595 Review.
-
Beyond RCHOP: A Blueprint for Diffuse Large B Cell Lymphoma Research.J Natl Cancer Inst. 2016 Dec 16;108(12):djw257. doi: 10.1093/jnci/djw257. Print 2016 Dec. J Natl Cancer Inst. 2016. PMID: 27986884 Free PMC article. Review.
Cited by
-
Validation of the Double-Hit Gene Expression Signature (DLBCL90) in an Independent Cohort of Patients with Diffuse Large B-Cell Lymphoma of Germinal Center Origin.J Mol Diagn. 2021 May;23(5):658-664. doi: 10.1016/j.jmoldx.2021.02.005. Epub 2021 Feb 23. J Mol Diagn. 2021. PMID: 33636392 Free PMC article.
-
Integrative genomic analysis focused on cell cycle genes for MYC-driven aggressive mature B-cell lymphoma.J Clin Exp Hematop. 2020;60(3):87-96. doi: 10.3960/jslrt.20021. J Clin Exp Hematop. 2020. PMID: 32981916 Free PMC article.
-
Prognostic Significance of Diffuse Large B-Cell Lymphoma Cell of Origin Determined by Digital Gene Expression in Formalin-Fixed Paraffin-Embedded Tissue Biopsies.J Clin Oncol. 2015 Sep 10;33(26):2848-56. doi: 10.1200/JCO.2014.60.2383. Epub 2015 Aug 3. J Clin Oncol. 2015. PMID: 26240231 Free PMC article.
-
Different biological risk factors in young poor-prognosis and elderly patients with diffuse large B-cell lymphoma.Leukemia. 2015 Jul;29(7):1564-70. doi: 10.1038/leu.2015.43. Epub 2015 Feb 17. Leukemia. 2015. PMID: 25687653
-
Using Gene Expression Profiling to Move Beyond MYC/BCL2 Rearrangements in High-Grade Lymphoma.J Clin Oncol. 2019 Jan 20;37(3):175-177. doi: 10.1200/JCO.18.01910. Epub 2018 Dec 3. J Clin Oncol. 2019. PMID: 30523718 Free PMC article. No abstract available.
References
-
- Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC Press; 2008. pp. 265–266.
-
- Alizadeh AA, Eisen MB, Davis RE, et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000;403:503–511. - PubMed
-
- Hans CP, Weisenburger DD, Greiner TC, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004;103:275–282. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
