

Minimally invasive liver resection to obtain tumor-infiltrating lymphocytes for adoptive cell therapy in patients with metastatic melanoma
- PMID: 22726267
- PMCID: PMC3408344
- DOI: 10.1186/1477-7819-10-113
Minimally invasive liver resection to obtain tumor-infiltrating lymphocytes for adoptive cell therapy in patients with metastatic melanoma
Abstract
Background: Adoptive cell therapy (ACT) with tumor-infiltrating lymphocytes (TIL) in patients with metastatic melanoma has been reported to have a 56% overall response rate with 20% complete responders. To increase the availability of this promising therapy in patients with advanced melanoma, a minimally invasive approach to procure tumor for TIL generation is warranted.
Methods: A feasibility study was performed to determine the safety and efficacy of laparoscopic liver resection to generate TIL for ACT. Retrospective review of a prospectively maintained database identified 22 patients with advanced melanoma and visceral metastasis (AJCC Stage M1c) who underwent laparoscopic liver resection between 1 October 2005 and 31 July 2011. The indication for resection in all patients was to receive postoperative ACT with TIL.
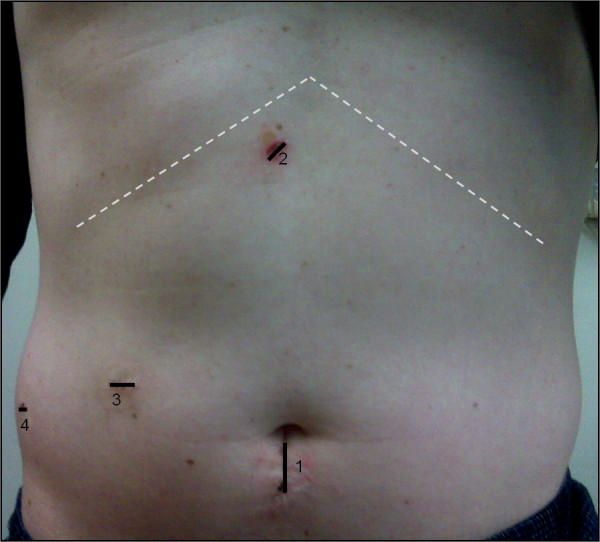
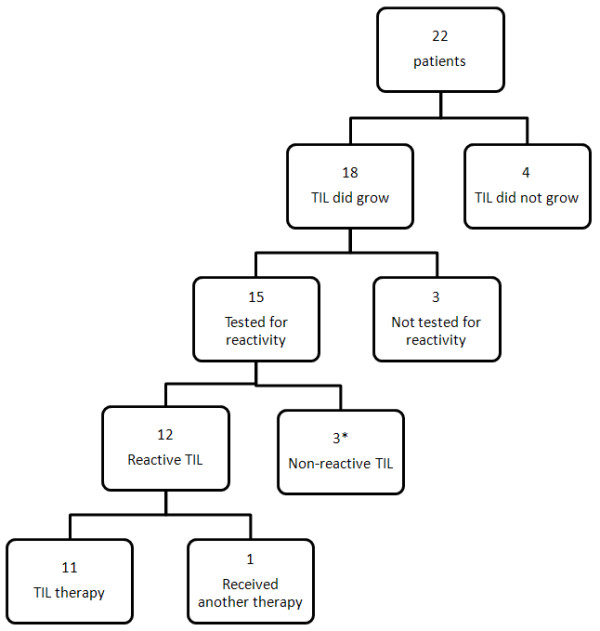
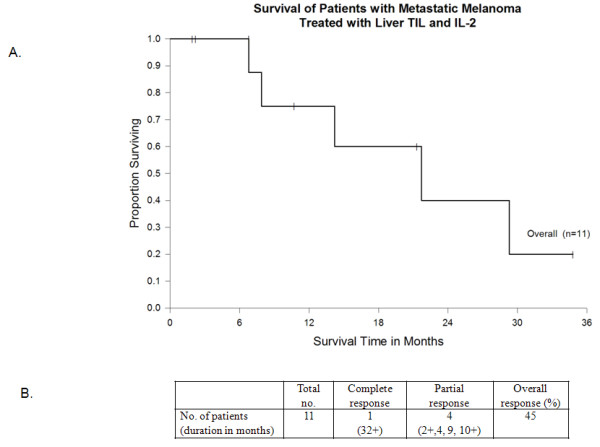
Results: Twenty patients (91%) underwent resection utilizing a closed laparoscopic technique, one required hand-assistance and another required conversion to open resection. Median intraoperative blood loss was 100 mL with most cases performed without a Pringle maneuver. Median hospital stay was 3 days. Three (14%) patients experienced a complication from resection with no mortality. TIL were generated from 18 of 22 (82%) patients. Twelve of 15 (80%) TIL tested were found to have in vitro tumor reactivity. Eleven patients (50%) received the intended ACT. Two patients were rendered no evidence of disease after surgical resection, with one undergoing delayed ACT with generated TIL after relapse. Objective tumor response was seen in 5 of 11 patients (45%) who received TIL, with one patient experiencing an ongoing complete response (32+ months).
Conclusions: Laparoscopic liver resection can be performed with minimal morbidity and serve as an effective means to procure tumor to generate therapeutic TIL for ACT to patients with metastatic melanoma.
Figures
Similar articles
-
Liver resection for metastatic melanoma with postoperative tumor-infiltrating lymphocyte therapy.Ann Surg Oncol. 2010 Jan;17(1):163-70. doi: 10.1245/s10434-009-0677-0. Epub 2009 Sep 24. Ann Surg Oncol. 2010. PMID: 19777192 Free PMC article.
-
Clinical responses in a phase II study using adoptive transfer of short-term cultured tumor infiltration lymphocytes in metastatic melanoma patients.Clin Cancer Res. 2010 May 1;16(9):2646-55. doi: 10.1158/1078-0432.CCR-10-0041. Epub 2010 Apr 20. Clin Cancer Res. 2010. PMID: 20406835 Clinical Trial.
-
Adoptive immunotherapy with tumor-infiltrating lymphocytes and interleukin-2 in patients with metastatic malignant melanoma and renal cell carcinoma: a pilot study.J Clin Oncol. 1995 Aug;13(8):1939-49. doi: 10.1200/JCO.1995.13.8.1939. J Clin Oncol. 1995. PMID: 7636534 Clinical Trial.
-
Tumor-infiltrating lymphocytes in melanoma.Curr Oncol Rep. 2012 Oct;14(5):468-74. doi: 10.1007/s11912-012-0257-5. Curr Oncol Rep. 2012. PMID: 22878966 Free PMC article. Review.
-
White paper on adoptive cell therapy for cancer with tumor-infiltrating lymphocytes: a report of the CTEP subcommittee on adoptive cell therapy.Clin Cancer Res. 2011 Apr 1;17(7):1664-73. doi: 10.1158/1078-0432.CCR-10-2272. Epub 2011 Feb 15. Clin Cancer Res. 2011. PMID: 21325070 Review.
Cited by
-
Metastasectomy for Tumor-Infiltrating Lymphocytes: An Emerging Operative Indication in Surgical Oncology.Ann Surg Oncol. 2018 Feb;25(2):565-572. doi: 10.1245/s10434-017-6266-8. Epub 2017 Nov 29. Ann Surg Oncol. 2018. PMID: 29188500 Free PMC article.
-
Laparoscopic liver resection for metastatic melanoma.Surg Endosc. 2018 Mar;32(3):1470-1477. doi: 10.1007/s00464-017-5834-0. Epub 2017 Sep 15. Surg Endosc. 2018. PMID: 28916919
-
Partial hepatectomy for primary hepatic melanoma: a report of two cases and review of the literature.World J Surg Oncol. 2014 Nov 28;12:362. doi: 10.1186/1477-7819-12-362. World J Surg Oncol. 2014. PMID: 25430016 Free PMC article. Review.
-
Efficacy of Tumor-Infiltrating Lymphocytes Combined with IFN-α in Chinese Resected Stage III Malignant Melanoma.J Immunol Res. 2017;2017:1092507. doi: 10.1155/2017/1092507. Epub 2017 Aug 20. J Immunol Res. 2017. PMID: 28913367 Free PMC article.
-
Surgical Considerations for Tumor Tissue Procurement to Obtain Tumor-Infiltrating Lymphocytes for Adoptive Cell Therapy.Cancer J. 2022 Jul-Aug 01;28(4):285-293. doi: 10.1097/PPO.0000000000000608. Cancer J. 2022. PMID: 35880938 Free PMC article. Review.
References
-
- Balch CM, Soong SJ, Gershenwald JE, Thompson JF, Reintgen DS, Cascinelli N, Urist M, McMasters KM, Ross MI, Kirkwood JM, Atkins MB, Thompson JA, Coit DG, Byrd D, Desmond R, Zhang Y, Liu PY, Lyman GH, Morabito A. Prognostic factors analysis of 17,600 melanoma patients: validation of the American Joint Committee on Cancer melanoma staging system. J Clin Oncol. 2001;19:3622–3634. - PubMed
-
- Barth A, Wanek LA, Morton DL. Prognostic factors in 1,521 melanoma patients with distant metastases. J Am Coll Surg. 1995;181:193–201. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
