

Umbilical cord blood levels of maternal antibodies reactive with p200 and full-length Ro 52 in the assessment of risk for cardiac manifestations of neonatal lupus
- PMID: 22511615
- PMCID: PMC3413772
- DOI: 10.1002/acr.21704
Umbilical cord blood levels of maternal antibodies reactive with p200 and full-length Ro 52 in the assessment of risk for cardiac manifestations of neonatal lupus
Abstract
Objective: Maternal anti-Ro autoantibodies are associated with cardiac manifestations of neonatal lupus (cardiac NL), yet only 2% of women with this reactivity have an affected child. Identification of a more specific marker would channel intense monitoring to fetuses at greater risk. This study aimed to determine whether autoantibodies against Ro 52 amino acids 200-239 (p200) confer added risk over autoantibodies to full-length Ro 52, Ro 60, or La.
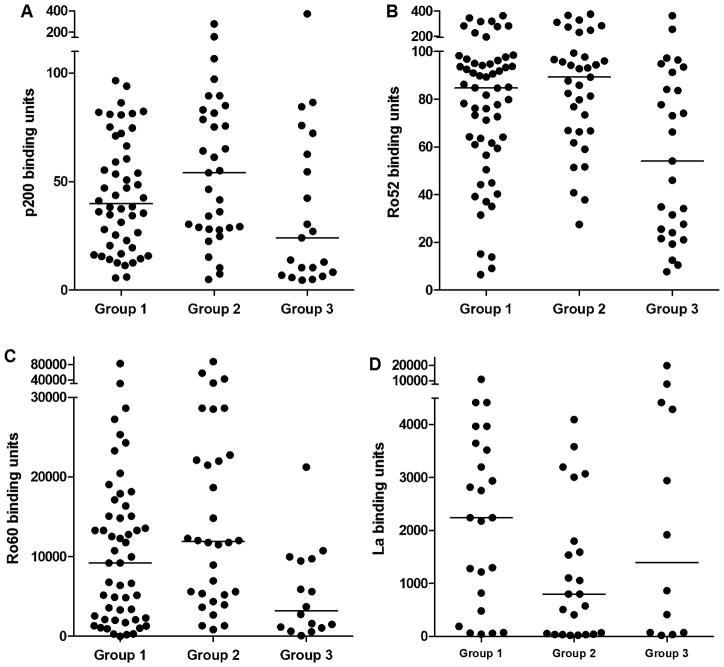
Methods: Anti-Ro-exposed pregnancies resulting in cardiac NL or no cardiac manifestations were identified from the Research Registry for Neonatal Lupus and the PR Interval and Dexamethasone Evaluation study. Umbilical cord (n = 123) and maternal (n = 115) samples were evaluated by enzyme-linked immunosorbent assay.
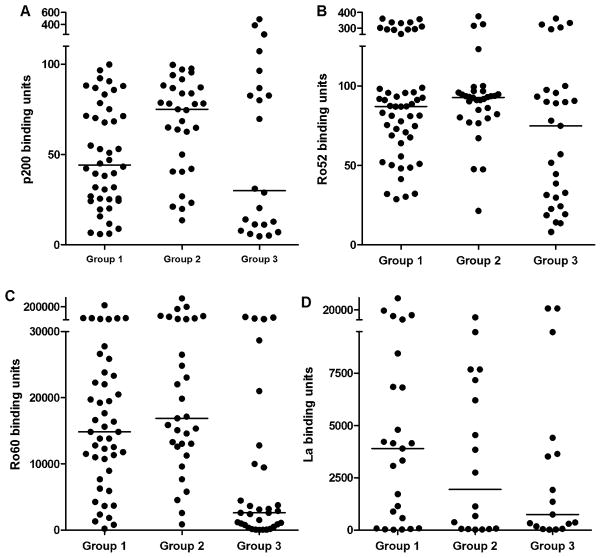
Results: The frequencies of p200, Ro 52, Ro 60, and La autoantibodies were not significantly different between affected and unaffected children. However, neonatal anti-Ro 52 and Ro 60 titers were highest in cardiac NL and their unaffected siblings compared to unaffected neonates without a cardiac NL sibling. Although both maternal anti-Ro 52 and p200 autoantibodies were less than 50% specific for cardiac NL, anti-p200 was the least likely of the Ro autoantibodies to be false-positive in mothers who have never had an affected child. Titers of anti-Ro 52 and p200 did not differ during a cardiac NL or unaffected pregnancy from the same mother.
Conclusion: Maternal reactivity to p200 does not confer an added risk to fetal conduction defects over full-length Ro 52 or Ro 60 autoantibodies. Mothers who may never be at risk for having an affected child have lower anti-Ro 60 titers and may require less stringent echocardiographic monitoring compared to women with high-titer autoantibodies.
Copyright © 2012 by the American College of Rheumatology.
Figures
Similar articles
-
Maternal antibody responses to the 52-kd SSA/RO p200 peptide and the development of fetal conduction defects.Arthritis Rheum. 2005 Oct;52(10):3079-86. doi: 10.1002/art.21289. Arthritis Rheum. 2005. PMID: 16200587
-
Anti-Ro/SSA-p200 antibodies in the prediction of congenital heart block. An Italian multicentre cross-sectional study on behalf of the 'Forum Interdisciplinare per la Ricerca nelle Malattie Autoimmuni (FIRMA) Group'.Clin Exp Rheumatol. 2014 Nov-Dec;32(6):848-54. Epub 2014 Oct 20. Clin Exp Rheumatol. 2014. PMID: 25327946
-
A central role of plasmin in cardiac injury initiated by fetal exposure to maternal anti-Ro autoantibodies.Rheumatology (Oxford). 2013 Aug;52(8):1448-53. doi: 10.1093/rheumatology/ket156. Epub 2013 Apr 18. Rheumatology (Oxford). 2013. PMID: 23598443 Free PMC article.
-
Neonatal lupus: bedside to bench and back.Scand J Rheumatol. 1996;25(5):271-6. doi: 10.3109/03009749609104057. Scand J Rheumatol. 1996. PMID: 8921918 Review.
-
[Neonatal lupus erythematosus].Nihon Rinsho Meneki Gakkai Kaishi. 2017;40(2):124-130. doi: 10.2177/jsci.40.124. Nihon Rinsho Meneki Gakkai Kaishi. 2017. PMID: 28603203 Review. Japanese.
Cited by
-
In search of an antibody specificity highly predictive of congenital heart block.Lupus Sci Med. 2016 Apr 21;3(1):e000154. doi: 10.1136/lupus-2016-000154. eCollection 2016. Lupus Sci Med. 2016. PMID: 27158527 Free PMC article. No abstract available.
-
Progress in the pathogenesis and treatment of cardiac manifestations of neonatal lupus.Curr Opin Rheumatol. 2017 Sep;29(5):467-472. doi: 10.1097/BOR.0000000000000414. Curr Opin Rheumatol. 2017. PMID: 28520682 Free PMC article. Review.
-
Modulation of natural IgM autoantibodies to oxidative stress-related neo-epitopes on apoptotic cells in newborns of mothers with anti-Ro autoimmunity.J Autoimmun. 2016 Sep;73:30-41. doi: 10.1016/j.jaut.2016.05.014. Epub 2016 Jun 8. J Autoimmun. 2016. PMID: 27289167 Free PMC article.
-
Ro52 autoantibodies arise from self-reactive progenitors in a mother of a child with neonatal lupus.J Autoimmun. 2017 May;79:99-104. doi: 10.1016/j.jaut.2017.01.004. Epub 2017 Jan 22. J Autoimmun. 2017. PMID: 28118945 Free PMC article.
-
Autoantibody-mediated impairment of DNASE1L3 activity in sporadic systemic lupus erythematosus.J Exp Med. 2021 May 3;218(5):e20201138. doi: 10.1084/jem.20201138. J Exp Med. 2021. PMID: 33783474 Free PMC article.
References
-
- Buyon JP, Friedman DM. Neonatal Lupus. In: Lahita RG, Tsokos G, Buyon JP, Koike T, editors. Systemic Lupus Erythematosus. 5. San Diego: Academic Press; 2011. pp. 541–67.
-
- Friedman DM, Kim MY, Copel JA, Davis C, Phoon CK, Glickstein JS, et al. Utility of cardiac monitoring in fetuses at risk for congenital heart block: the PR Interval and Dexamethasone Evaluation (PRIDE) prospective study. Circulation. 2008;117:485–93. - PubMed
-
- Buyon JP, Clancy RM. Neonatal Lupus: Basic Research and Clinical Perspectives. Rheum Dis Clin N Am. 2005;31:299–313. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
