

Cellular-based immunotherapies for patients with glioblastoma multiforme
- PMID: 22474481
- PMCID: PMC3299309
- DOI: 10.1155/2012/764213
Cellular-based immunotherapies for patients with glioblastoma multiforme
Abstract
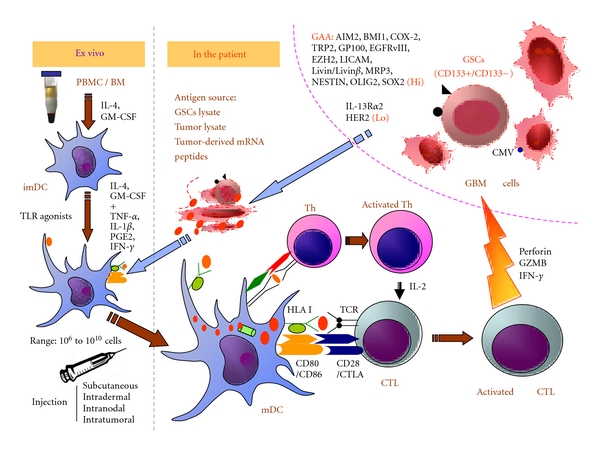
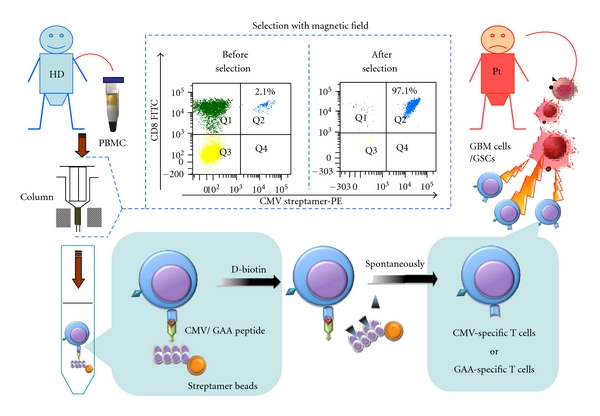
Treatment of patients with glioblastoma multiforme (GBM) remains to be a challenge with a median survival of 14.6 months following diagnosis. Standard treatment options include surgery, radiation therapy, and systemic chemotherapy with temozolomide. Despite the fact that the brain constitutes an immunoprivileged site, recent observations after immunotherapies with lysate from autologous tumor cells pulsed on dendritic cells (DCs), peptides, protein, messenger RNA, and cytokines suggest an immunological and even clinical response from immunotherapies. Given this plethora of immunomodulatory therapies, this paper gives a structure overview of the state-of-the art in the field. Particular emphasis was also put on immunogenic antigens as potential targets for a more specific stimulation of the immune system against GBM.
Figures
Similar articles
-
Immune response in patients with newly diagnosed glioblastoma multiforme treated with intranodal autologous tumor lysate-dendritic cell vaccination after radiation chemotherapy.J Immunother. 2011 May;34(4):382-9. doi: 10.1097/CJI.0b013e318215e300. J Immunother. 2011. PMID: 21499132 Free PMC article. Clinical Trial.
-
A phase II trial of autologous dendritic cell vaccination and radiochemotherapy following fluorescence-guided surgery in newly diagnosed glioblastoma patients.J Transl Med. 2017 May 12;15(1):104. doi: 10.1186/s12967-017-1202-z. J Transl Med. 2017. PMID: 28499389 Free PMC article. Clinical Trial.
-
Integration of autologous dendritic cell-based immunotherapy in the primary treatment for patients with newly diagnosed glioblastoma multiforme: a pilot study.J Neurooncol. 2010 Sep;99(2):261-72. doi: 10.1007/s11060-010-0131-y. Epub 2010 Feb 10. J Neurooncol. 2010. PMID: 20146084
-
Current vaccine trials in glioblastoma: a review.J Immunol Res. 2014;2014:796856. doi: 10.1155/2014/796856. Epub 2014 Apr 3. J Immunol Res. 2014. PMID: 24804271 Free PMC article. Review.
-
The evolution of the EGFRvIII (rindopepimut) immunotherapy for glioblastoma multiforme patients.Hum Vaccin Immunother. 2014;10(11):3322-31. doi: 10.4161/21645515.2014.983002. Hum Vaccin Immunother. 2014. PMID: 25625931 Free PMC article. Review.
Cited by
-
Potential Molecular Mechanism of TNF Superfamily-Related Genes in Glioblastoma Multiforme Based on Transcriptome and Epigenome.Front Neurol. 2021 Feb 11;12:576382. doi: 10.3389/fneur.2021.576382. eCollection 2021. Front Neurol. 2021. PMID: 33643183 Free PMC article.
-
Assessment of genetic markers and glioblastoma stem-like cells in activation of dendritic cells.Hum Cell. 2013 Sep;26(3):105-13. doi: 10.1007/s13577-013-0065-8. Epub 2013 Jun 5. Hum Cell. 2013. PMID: 23737374
-
Probing the Bi-directional Interaction Between Microglia and Gliomas in a Tumor Microenvironment on a Microdevice.Neurochem Res. 2017 May;42(5):1478-1487. doi: 10.1007/s11064-017-2204-1. Epub 2017 Feb 24. Neurochem Res. 2017. PMID: 28236212
-
Clinical efficacy of tumor antigen-pulsed DC treatment for high-grade glioma patients: evidence from a meta-analysis.PLoS One. 2014 Sep 12;9(9):e107173. doi: 10.1371/journal.pone.0107173. eCollection 2014. PLoS One. 2014. PMID: 25215607 Free PMC article.
-
Dendritic cell vaccination combined with temozolomide retreatment: results of a phase I trial in patients with recurrent glioblastoma multiforme.J Neurooncol. 2015 Jan;121(2):319-29. doi: 10.1007/s11060-014-1635-7. Epub 2014 Oct 31. J Neurooncol. 2015. PMID: 25366363 Clinical Trial.
References
-
- Fleury A, Menegoz F, Grosclaude P, et al. Descriptive epidemiology of cerebral gliomas in France. Cancer. 1997;79(6):1195–1202. - PubMed
-
- Mirimanoff RO, Gorlia T, Mason W, et al. Radiotherapy and temozolomide for newly diagnosed glioblastoma: recursive partitioning analysis of the EORTC 26981/22981-NCIC CE3 phase III randomized trial. Journal of Clinical Oncology. 2006;24(16):2563–2569. - PubMed
-
- Stummer W, Reulen HJ, Meinel T, et al. Extent of resection and survival in glioblastoma multiforme: identification of and adjustment for bias. Neurosurgery. 2008;62(3):564–576. - PubMed
-
- Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Reulen HJ. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. The Lancet Oncology. 2006;7(5):392–401. - PubMed
-
- Stockhammer F, Misch M, Horn P, Koch A, Fonyuy N, Plotkin M. Association of F18-fluoro-ethyl-tyrosin uptake and 5-aminolevulinic acid-induced fluorescence in gliomas. Acta Neurochirurgica. 2009;151(11):1377–1383. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
