

Lessons from a one-year hospital-based surveillance of acute respiratory infections in Berlin- comparing case definitions to monitor influenza
- PMID: 22452874
- PMCID: PMC3362781
- DOI: 10.1186/1471-2458-12-245
Lessons from a one-year hospital-based surveillance of acute respiratory infections in Berlin- comparing case definitions to monitor influenza
Abstract
Background: Surveillance of severe acute respiratory infections (SARI) in sentinel hospitals is recommended to estimate the burden of severe influenza-cases. Therefore, we monitored patients admitted with respiratory infections (RI) in 9 Berlin hospitals from 7.12.2009 to 12.12.2010 according to different case definitions (CD) and determined the proportion of cases with influenza A(H1N1)pdm09 (pH1N1). We compared the sensitivity and specificity of CD for capturing pandemic pH1N1 cases.
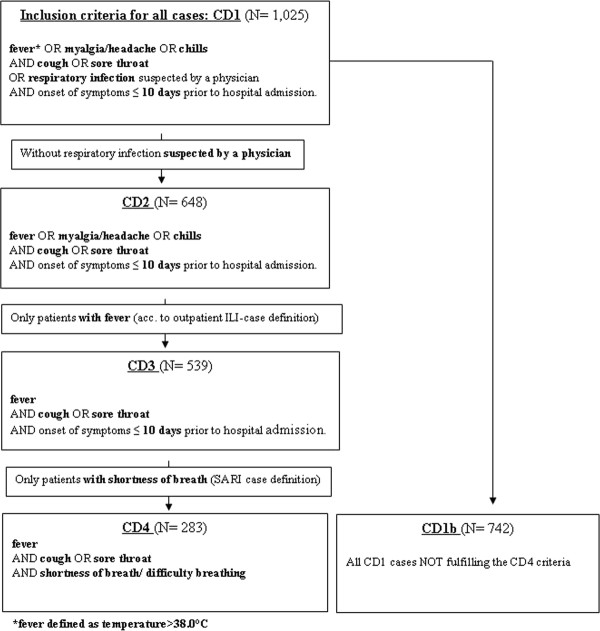
Methods: We established an RI-surveillance restricted to adults aged ≤ 65 years within the framework of a pH1N1 vaccine effectiveness study, which required active identification of RI-cases. The hospital information-system was screened daily for newly admitted RI-patients. Nasopharyngeal swabs from consenting patients were tested by PCR for influenza-virus subtypes. Four clinical CD were compared in terms of capturing pH1N1-positives among hospitalized RI-patients by applying sensitivity and specificity analyses. The broadest case definition (CD1) was used for inclusion of RI-cases; the narrowest case definition (CD4) was identical to the SARI case definition recommended by ECDC/WHO.
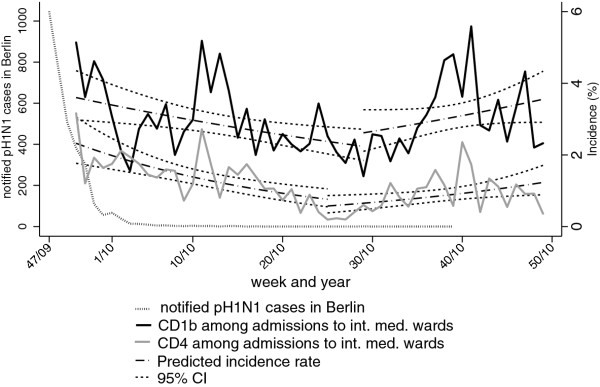
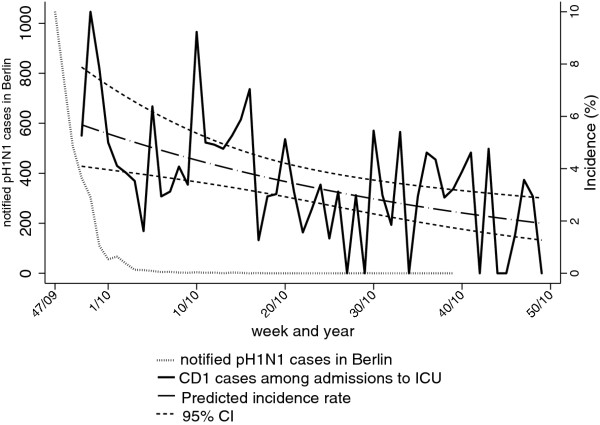
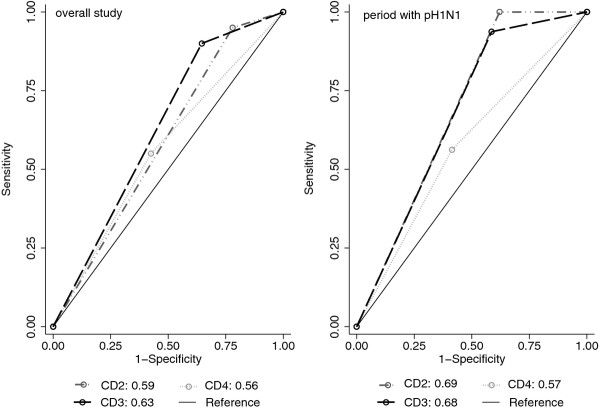
Results: Over the study period, we identified 1,025 RI-cases, of which 283 (28%) met the ECDC/WHO SARI case definition. The percentage of SARI-cases among internal medicine admissions decreased from 3.2% (calendar-week 50-2009) to 0.2% (week 25-2010). Of 354 patients tested by PCR, 20 (6%) were pH1N1-positive. Two case definitions narrower than CD1 but -in contrast to SARI- not requiring shortness of breath yielded the largest areas under the Receiver-Operator-Curve. Heterogeneity of proportions of patients admitted with RI between hospitals was significant.
Conclusions: Comprehensive surveillance of RI cases was feasible in a network of community hospitals. In most settings, several hospitals should be included to ensure representativeness. Although misclassification resulting from failure to obtain symptoms in the hospital information-system cannot be ruled out, a high proportion of hospitalized PCR-positive pH1N1-patients (45%) did not fulfil the SARI case-definition that included shortness of breath or difficulty breathing. Thus, to assess influenza-related disease burden in hospitals, broader, alternative case definitions should be considered.
Figures
Similar articles
-
Sentinel surveillance for influenza among severe acute respiratory infection and acute febrile illness inpatients at three hospitals in Ghana.Influenza Other Respir Viruses. 2016 Sep;10(5):367-74. doi: 10.1111/irv.12397. Epub 2016 Jun 30. Influenza Other Respir Viruses. 2016. PMID: 27239956 Free PMC article.
-
Prospective hospital-based case-control study to assess the effectiveness of pandemic influenza A(H1N1)pdm09 vaccination and risk factors for hospitalization in 2009-2010 using matched hospital and test-negative controls.BMC Infect Dis. 2012 May 31;12:127. doi: 10.1186/1471-2334-12-127. BMC Infect Dis. 2012. PMID: 22650369 Free PMC article.
-
[Estimating the burden of influenza-associated hospitalization for cases of severe acute respiratory infection, Beijing, 2015].Zhonghua Yu Fang Yi Xue Za Zhi. 2017 Dec 6;51(12):1097-1101. doi: 10.3760/cma.j.issn.0253-9624.2017.12.009. Zhonghua Yu Fang Yi Xue Za Zhi. 2017. PMID: 29262491 Chinese.
-
Influenza and HIV: lessons from the 2009 H1N1 influenza pandemic.Curr HIV/AIDS Rep. 2011 Sep;8(3):181-91. doi: 10.1007/s11904-011-0086-4. Curr HIV/AIDS Rep. 2011. PMID: 21710214 Review.
-
Is influenza-like illness a useful concept and an appropriate test of influenza vaccine effectiveness?Vaccine. 2014 Apr 17;32(19):2143-9. doi: 10.1016/j.vaccine.2014.02.059. Epub 2014 Feb 28. Vaccine. 2014. PMID: 24582634 Free PMC article. Review.
Cited by
-
The East Jakarta Project: surveillance for highly pathogenic avian influenza A(H5N1) and seasonal influenza viruses in patients seeking care for respiratory disease, Jakarta, Indonesia, October 2011-September 2012.Epidemiol Infect. 2015 Dec;143(16):3394-404. doi: 10.1017/S0950268815000771. Epub 2015 Apr 27. Epidemiol Infect. 2015. PMID: 25912029 Free PMC article.
-
Southern Hemisphere Influenza and Vaccine Effectiveness Research and Surveillance.Influenza Other Respir Viruses. 2015 Jul;9(4):179-90. doi: 10.1111/irv.12315. Influenza Other Respir Viruses. 2015. PMID: 25912617 Free PMC article. Review.
-
Infection surveillance measures during the COVID-19 pandemic in Germany.GMS Hyg Infect Control. 2021 Sep 14;16:Doc27. doi: 10.3205/dgkh000398. eCollection 2021. GMS Hyg Infect Control. 2021. PMID: 34650903 Free PMC article. Review.
-
Influenza B-cells protective epitope characterization: a passkey for the rational design of new broad-range anti-influenza vaccines.Viruses. 2012 Nov 14;4(11):3090-108. doi: 10.3390/v4113090. Viruses. 2012. PMID: 23202517 Free PMC article. Review.
-
Establishing an ICD-10 code based SARI-surveillance in Germany - description of the system and first results from five recent influenza seasons.BMC Public Health. 2017 Jun 30;17(1):612. doi: 10.1186/s12889-017-4515-1. BMC Public Health. 2017. PMID: 28666433 Free PMC article.
References
-
- Arbeitsgemeinschaft Influenza (AGI) Bericht zur Epidemiologie der Influenza in Deutschland Saison 2009/10. 2010.
-
- Rothberg MB, Haessler SD. Complications of seasonal and pandemic influenza. Crit Care Med. 2010;38(4 Suppl):e91–97. - PubMed
-
- Baker MG, Wilson N, Huang QS, Paine S, Lopez L, Bandaranayake D, Tobias M, Mason K, Mackereth GF, Jacobs M, Thornley C, Roberts S, McArthur C. Pandemic influenza A(H1N1)v in New Zealand: the experience from April to August 2009. Euro Surveill. 2009;14(34) pii = 19319 http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19319. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
