

PET/CT in the management of patients with stage IIIC and IV metastatic melanoma considered candidates for surgery: evaluation of the additive value after conventional imaging
- PMID: 22451559
- PMCID: PMC3880209
- DOI: 10.2214/AJR.11.7280
PET/CT in the management of patients with stage IIIC and IV metastatic melanoma considered candidates for surgery: evaluation of the additive value after conventional imaging
Abstract
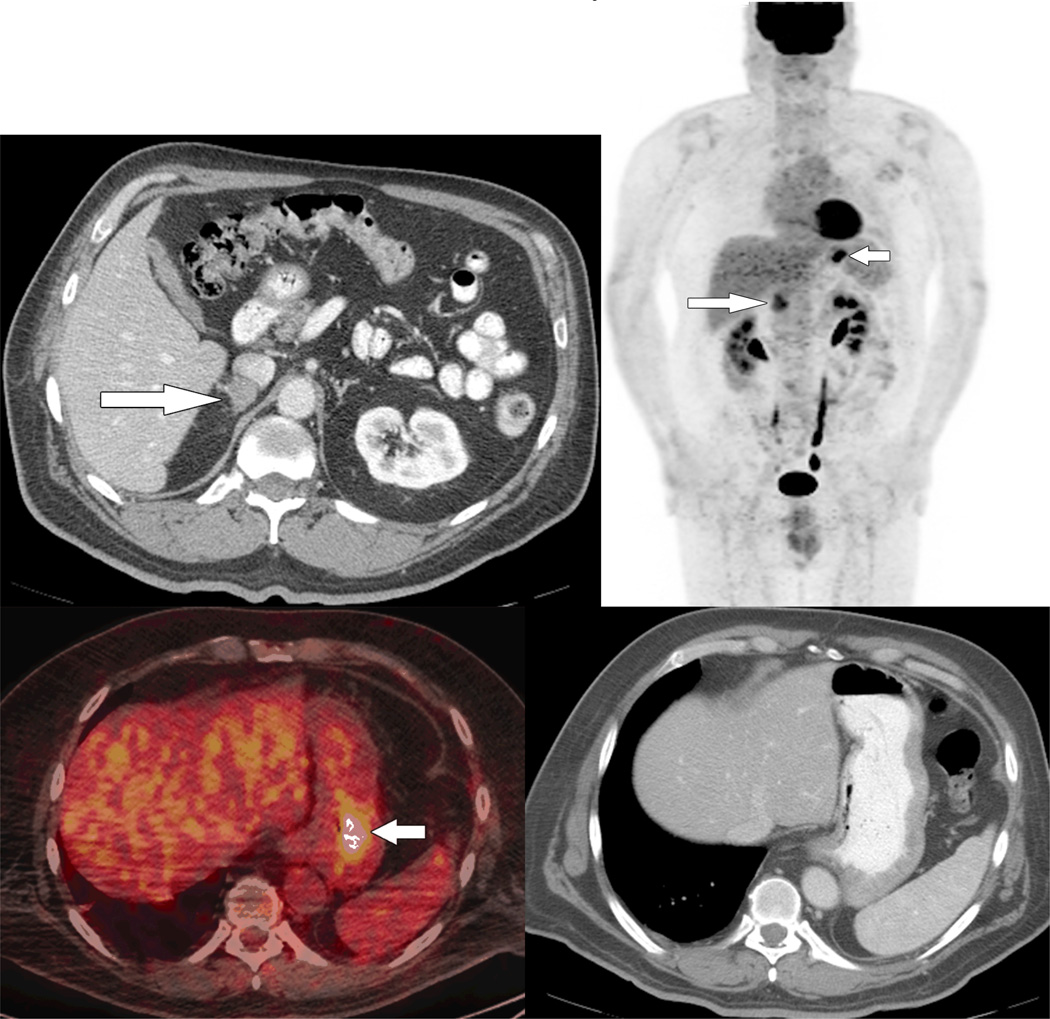
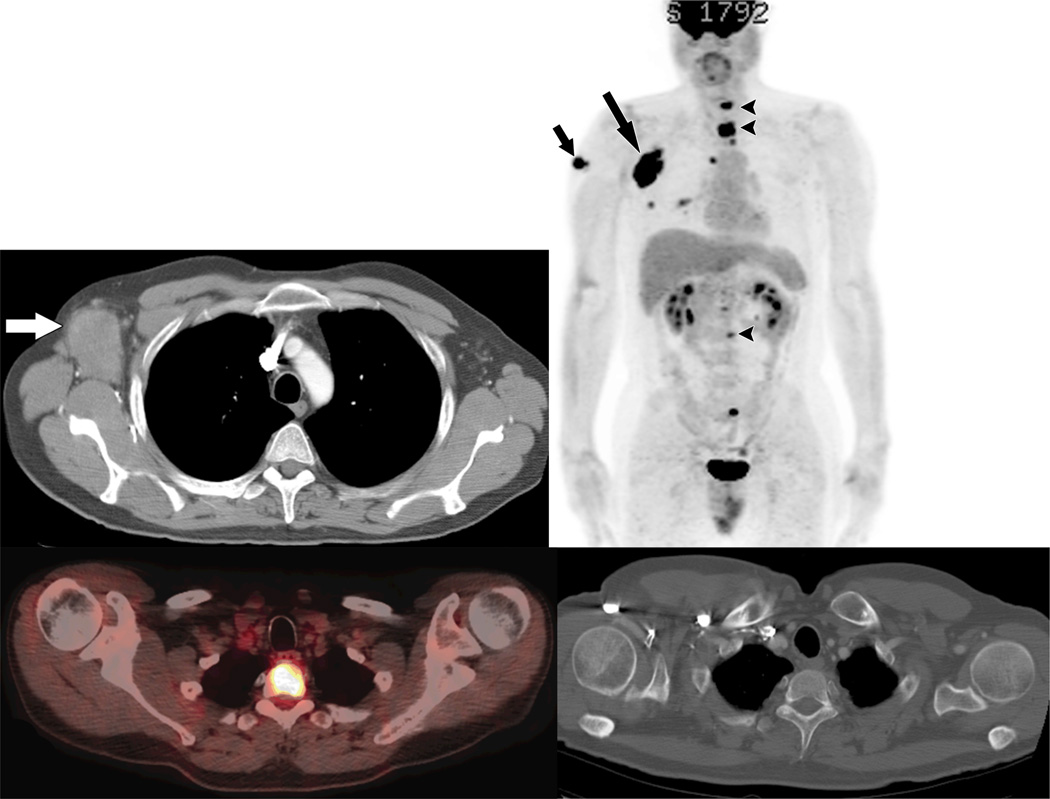
Objective: The purpose of this article is to determine how often unexpected (18)F-FDG PET/CT findings result in a change in management for patients with stage IV and clinically evident stage III melanoma with resectable disease according to conventional imaging.
Subjects and methods: Thirty-two patients with oligometastatic stage IV and clinically evident stage III melanoma were identified by surgical oncologists according to the results of conventional imaging, which included contrast-enhanced CT of the chest, abdomen, and pelvis and MRI of the brain. The surgical plan included resection of known metastases or isolated limb perfusion with chemotherapy. Thirty-three FDG PET/CT scans were performed within 36 days of their contrast-enhanced CT. The impact of PET/CT was defined as the percentage of cases in which a change in the surgical plan resulted from the unanticipated PET/CT findings.
Results: PET/CT revealed unexpected melanoma metastases in 12% of scans (4/33). As a result, the surgery was canceled for two patients, and the planned approach was altered for another two patients to address the unexpected sites. In 6% of scans (2/33), the unexpected metastases were detected in the extremities, which were not included in conventional imaging. Three scans (9%) showed false-positive FDG-avid findings that proved to be benign by subsequent stability or resolution with no therapy.
Conclusion: In patients with surgically treatable metastatic melanoma, FDG PET/CT can detect unexpected metastases that are missed or not imaged with conventional imaging, and can be considered as part of preoperative workup.
Figures

Similar articles
-
Influence of (18)F-FDG PET/CT on therapy management in patients with stage III/IV malignant melanoma.Eur J Nucl Med Mol Imaging. 2016 Mar;43(3):482-8. doi: 10.1007/s00259-015-3187-2. Epub 2015 Sep 18. Eur J Nucl Med Mol Imaging. 2016. PMID: 26384681
-
A multicenter prospective evaluation of the clinical utility of F-18 FDG-PET/CT in patients with AJCC stage IIIB or IIIC extremity melanoma.Ann Surg. 2012 Aug;256(2):350-6. doi: 10.1097/SLA.0b013e318256d1f5. Ann Surg. 2012. PMID: 22691370 Free PMC article.
-
[Impact of whole body magnetic resonance imaging (MRI) in the management of melanoma patients, in comparison with positron emission tomography/computed tomography (TEP/CT) and CT].Ann Dermatol Venereol. 2011 May;138(5):377-83. doi: 10.1016/j.annder.2011.02.023. Epub 2011 Apr 22. Ann Dermatol Venereol. 2011. PMID: 21570561 Clinical Trial. French.
-
Clinical applications of fluorodeoxyglucose--positron emission tomography in the management of malignant melanoma.Curr Opin Oncol. 2005 Mar;17(2):154-9. doi: 10.1097/01.cco.0000152626.98124.3a. Curr Opin Oncol. 2005. PMID: 15725921 Review.
-
Fluorodeoxyglucose-PET in the management of malignant melanoma.Radiol Clin North Am. 2005 Jan;43(1):23-33. doi: 10.1016/j.rcl.2004.09.011. Radiol Clin North Am. 2005. PMID: 15693645 Review.
Cited by
-
Ultrasound, CT, MRI, or PET-CT for staging and re-staging of adults with cutaneous melanoma.Cochrane Database Syst Rev. 2019 Jul 1;7(7):CD012806. doi: 10.1002/14651858.CD012806.pub2. Cochrane Database Syst Rev. 2019. PMID: 31260100 Free PMC article.
-
Diagnostic Accuracy and Impact of Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in Preoperative Staging of Cutaneous Malignant Melanoma: Results of a Prospective Study in Indian Population.World J Nucl Med. 2017 Oct-Dec;16(4):286-292. doi: 10.4103/1450-1147.215491. World J Nucl Med. 2017. PMID: 29033677 Free PMC article.
-
Liver resection and ablation for metastatic melanoma: A single center experience.J Surg Oncol. 2015 Jun;111(8):962-8. doi: 10.1002/jso.23929. Epub 2015 Jun 12. J Surg Oncol. 2015. PMID: 26073980 Free PMC article.
-
[Whole-body staging of malignant melanoma: advantages, limitations and current importance of PET-CT, whole-body MRI and PET-MRI].Radiologe. 2015 Feb;55(2):120-6. doi: 10.1007/s00117-014-2762-z. Radiologe. 2015. PMID: 25589421 German.
-
Influence of (18)F-FDG PET/CT on therapy management in patients with stage III/IV malignant melanoma.Eur J Nucl Med Mol Imaging. 2016 Mar;43(3):482-8. doi: 10.1007/s00259-015-3187-2. Epub 2015 Sep 18. Eur J Nucl Med Mol Imaging. 2016. PMID: 26384681
References
-
- Coit DG, Andtbacka R, Anker CJ, et al. NCCN Clinical Practice Guidelines in Oncology. National Comprehensive Cancer Network; 2011. Melanoma. - PubMed
-
- Choi EA, Gershenwald JE. Imaging studies in patients with melanoma. Surg Oncol Clin N Am. 2007;16:403–430. - PubMed
-
- Tyler DS, Onaitis M, Kherani A, et al. Positron emission tomography scanning in malignant melanoma. Cancer. 2000;89:1019–1025. - PubMed
-
- Miranda EP, Gertner M, Wall J, et al. Routine imaging of asymptomatic melanoma patients with metastasis to sentinel lymph nodes rarely identifies systemic disease. Arch Surg. 2004;139:831–836. discussion 836–837. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
