

Statin therapy as prevention against development of acute respiratory distress syndrome: an observational study
- PMID: 22430234
- PMCID: PMC3939937
- DOI: 10.1097/CCM.0b013e3182416d7a
Statin therapy as prevention against development of acute respiratory distress syndrome: an observational study
Abstract
Objectives: The 3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors ("statins") have anti-inflammatory properties and are associated with improved outcomes in critically ill patients. We investigated whether previous statin therapy affects outcomes in patients at risk for acute respiratory distress syndrome.
Design: Patients were followed-up for the primary outcome of acute respiratory distress syndrome and secondary outcomes of intensive care unit and 60-day mortality, organ dysfunction, and ventilator-free days in a secondary analysis of a prospective cohort study. Receipt of statin therapy was recorded. Propensity score matching was used to adjust for confounding by indication.
Setting: Intensive care units at a tertiary care academic medical center.
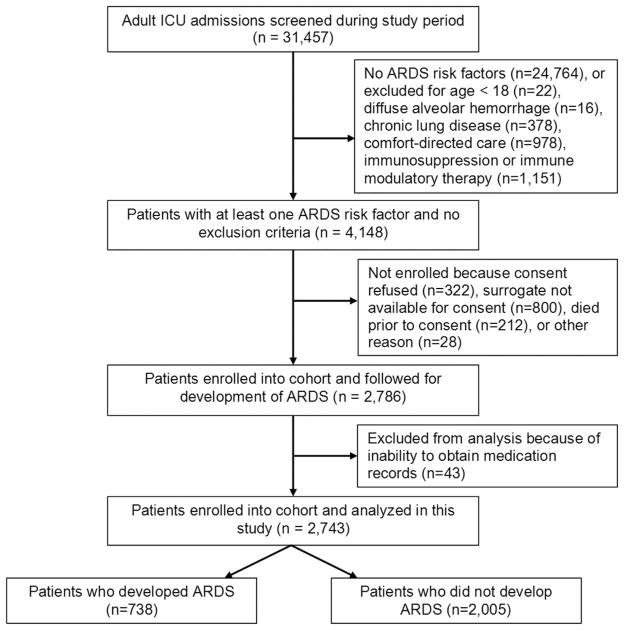
Patients: Critically ill patients (2,743) with acute respiratory distress syndrome risk factors.
Interventions: None.
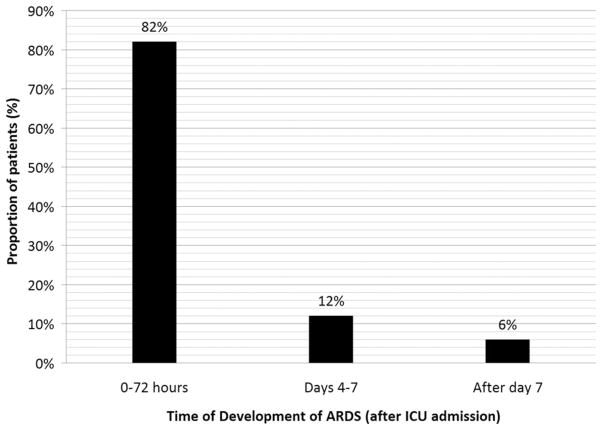
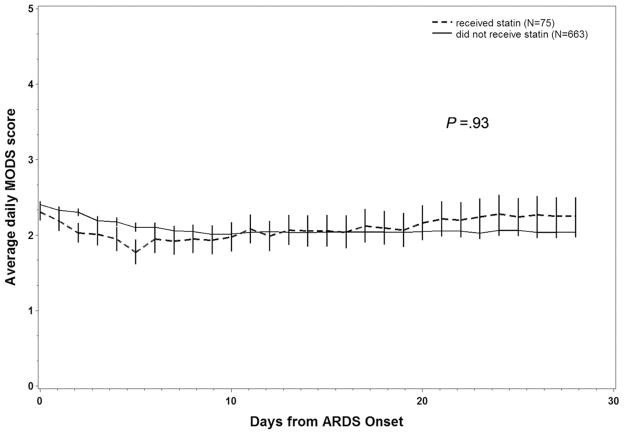
Measurements and main results: Acute respiratory distress syndrome developed in 738 (26%) patients; 413 patients (15%) received a statin within 24 hrs of intensive care unit admission. Those who had received a statin within 24 hrs had a lower rate of development of acute respiratory distress syndrome (odds ratio 0.56; 95% confidence interval 0.43-0.73; p<.0001). After multivariate adjustment for potential confounders, this association remained significant (odds ratio 0.69; 95% confidence interval 0.51-0.92; p=.01). However, after propensity score matching, the association was not statistically significant (odds ratio 0.79; 95% confidence interval 0.57-1.10; p=.16). Statin use was not associated with reduced acute respiratory distress syndrome mortality, organ dysfunction, or ventilator-free days. Results of the study were presented in accordance with STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
Conclusions: Statin therapy at the time of intensive care unit admission was not associated with a lower rate of development of acute respiratory distress syndrome after matching for patient propensity to receive statins. Statin therapy was not associated with improvements in acute respiratory distress syndrome mortality, organ failure, or days free from mechanical ventilation.
Conflict of interest statement
Dr. Malhotra has not disclosed any potential conflicts of interest.
Figures
Comment in
-
Statins and acute lung injury: Holy Grail or the next to fail?Crit Care Med. 2012 May;40(5):1661-3. doi: 10.1097/CCM.0b013e3182451fb2. Crit Care Med. 2012. PMID: 22511149 Free PMC article. No abstract available.
Similar articles
-
Impact of statin therapy on mortality in patients with sepsis-associated acute respiratory distress syndrome (ARDS) depends on ARDS severity: a prospective observational cohort study.BMC Med. 2015 Jun 1;13:128. doi: 10.1186/s12916-015-0368-6. BMC Med. 2015. PMID: 26033076 Free PMC article.
-
Prehospital statin and aspirin use and the prevalence of severe sepsis and acute lung injury/acute respiratory distress syndrome.Crit Care Med. 2011 Jun;39(6):1343-50. doi: 10.1097/CCM.0b013e3182120992. Crit Care Med. 2011. PMID: 21336116 Free PMC article.
-
Association between statin therapy and outcomes in critically ill patients: a nested cohort study.BMC Clin Pharmacol. 2011 Aug 6;11:12. doi: 10.1186/1472-6904-11-12. BMC Clin Pharmacol. 2011. PMID: 21819615 Free PMC article. Clinical Trial.
-
A case for continuing statin medications in the intensive care unit: Reducing the risk for delirium.Am J Health Syst Pharm. 2022 Aug 19;79(17):1431-1437. doi: 10.1093/ajhp/zxac132. Am J Health Syst Pharm. 2022. PMID: 35526279 Review.
-
Systematic Review and Meta-Analysis of Statin Use and Mortality, Intensive Care Unit Admission and Requirement for Mechanical Ventilation in COVID-19 Patients.J Clin Med. 2022 Sep 16;11(18):5454. doi: 10.3390/jcm11185454. J Clin Med. 2022. PMID: 36143101 Free PMC article. Review.
Cited by
-
Phenotypical and Functional Alteration of γδ T Lymphocytes in COVID-19 Patients: Reversal by Statins.Cells. 2022 Oct 31;11(21):3449. doi: 10.3390/cells11213449. Cells. 2022. PMID: 36359845 Free PMC article.
-
Statins and acute lung injury: Holy Grail or the next to fail?Crit Care Med. 2012 May;40(5):1661-3. doi: 10.1097/CCM.0b013e3182451fb2. Crit Care Med. 2012. PMID: 22511149 Free PMC article. No abstract available.
-
Statin use and Vital Organ Failure in Patients With Asthma-Chronic Obstructive Pulmonary Disease Overlap: A Time-Dependent Population-Based Study.Front Pharmacol. 2019 Aug 16;10:889. doi: 10.3389/fphar.2019.00889. eCollection 2019. Front Pharmacol. 2019. PMID: 31474854 Free PMC article.
-
Impact of prior statin therapy on the outcome of patients with suspected ventilator-associated pneumonia: an observational study.Crit Care. 2014 Apr 28;18(2):R83. doi: 10.1186/cc13845. Crit Care. 2014. PMID: 24774941 Free PMC article.
-
The upper and lower respiratory tract microbiome in severe aspiration pneumonia.iScience. 2023 May 6;26(6):106832. doi: 10.1016/j.isci.2023.106832. eCollection 2023 Jun 16. iScience. 2023. PMID: 37250794 Free PMC article.
References
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342:1334–1349. - PubMed
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353:1685–1693. - PubMed
-
- Stone NJ, Bilek S, Rosenbaum S. Recent National Cholesterol Education Program Adult Treatment Panel III update: Adjustments and options. Am J Cardiol. 2005;96:53E–59E. - PubMed
-
- Biasucci LM, Biasillo G, Stefanelli A. Inflammatory markers, cholesterol and statins: Pathophysiological role and clinical importance. Clin Chem Lab Med. 2010;48:1685–1691. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
