

Efficiency and risk factors for CMV transmission in seronegative hematopoietic stem cell recipients
- PMID: 22387334
- PMCID: PMC3572857
- DOI: 10.1016/j.bbmt.2012.02.008
Efficiency and risk factors for CMV transmission in seronegative hematopoietic stem cell recipients
Abstract
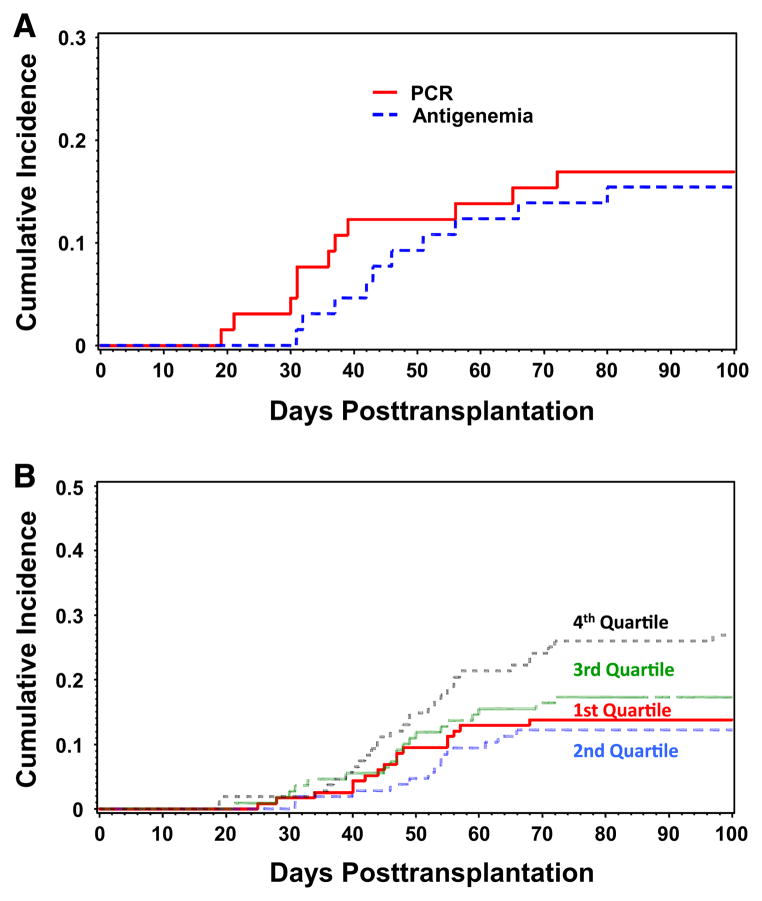
Cytomegalovirus (CMV) transmission via stem cells or marrow in CMV donor seropositive/recipient seronegative (D+/R-) hematopoietic cell transplantation (HCT) is surprisingly inefficient, and factors associated with transmission in these high-risk HCT recipients are unknown. In a retrospective cohort of D+/R- HCT recipients, cumulative incidence curve estimates were used to determine posttransplantation rates of CMV and multivariable Cox proportional models to assess risk factors associated with transmission. A total of 447 patients from 1995 to 2007 were eligible for enrollment. Overall, 85 of 447 (19.0%) acquired CMV at a median of 49 days (IQR 41-60) posttransplantation. CMV disease before day 100 occurred in 6 of 447 (1.3%) patients and in 7 of 447 (1.6%) after day 100. The donor graft, specifically the total nucleated cell count (adjusted hazard ratio [HR] 2.7; 95% confidence interval [CI], 1.4-4.7, P = .0002), was the only factor associated with CMV transmission in multivariable analyses. Notably, the source stem cells (marrow versus peripheral blood stem cell [PBSC]), screening method, and graft-versus-host disease (GVHD) were not associated with transmission. Thus, a highly cellular graft was the only identifiable risk factor associated with CMV transmission, suggesting that viral genomic content of the donor graft determines transmission efficiency in D+/R- HCT recipients.
Copyright © 2012 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
S.A.P. has received research support from Chimerix, Merck, Viropharma, and has been a consultant from Chimerix and Optimer Pharmaceuticals. M.J.B. has received research funding from Chimerix, Roche, Viropharma, and Vical and has been a consultant for Chimerix, Genentech, Roche, Vical, Novartis, Astellas, Boehringer Ingelheim, and Viropharma.
Figures

Similar articles
-
Risk factors for cytomegalovirus reactivation after CD6+ T-cell-depleted allogeneic bone marrow transplantation.Transplantation. 2002 Jul 15;74(1):49-54. doi: 10.1097/00007890-200207150-00009. Transplantation. 2002. PMID: 12134098
-
Incidence, risk factors, and outcome of cytomegalovirus viremia and gastroenteritis in patients with gastrointestinal graft-versus-host disease.Biol Blood Marrow Transplant. 2015 Jan;21(1):159-64. doi: 10.1016/j.bbmt.2014.10.004. Epub 2014 Oct 16. Biol Blood Marrow Transplant. 2015. PMID: 25445637 Free PMC article.
-
Cytomegalovirus Infection Incidence and Risk Factors Across Diverse Hematopoietic Cell Transplantation Platforms Using a Standardized Monitoring and Treatment Approach: A Comprehensive Evaluation from a Single Institution.Biol Blood Marrow Transplant. 2019 Mar;25(3):577-586. doi: 10.1016/j.bbmt.2018.10.011. Epub 2018 Oct 18. Biol Blood Marrow Transplant. 2019. PMID: 30342913 Free PMC article.
-
Emerging concepts in cytomegalovirus infection following hematopoietic stem cell transplantation.Hematol Oncol Stem Cell Ther. 2017 Dec;10(4):233-238. doi: 10.1016/j.hemonc.2017.05.001. Epub 2017 Jun 14. Hematol Oncol Stem Cell Ther. 2017. PMID: 28641094 Review.
-
Reexploring cytomegalovirus serology in allogeneic hematopoietic cell transplantation.Curr Opin Infect Dis. 2024 Aug 1;37(4):264-269. doi: 10.1097/QCO.0000000000001025. Epub 2024 Jun 10. Curr Opin Infect Dis. 2024. PMID: 38861267 Free PMC article. Review.
Cited by
-
Respiratory failure in the hematopoietic stem cell transplant recipient.World J Crit Care Med. 2018 Oct 16;7(5):62-72. doi: 10.5492/wjccm.v7.i5.62. eCollection 2018 Oct 16. World J Crit Care Med. 2018. PMID: 30370228 Free PMC article. Review.
-
CMV-specific T cells generated from naïve T cells recognize atypical epitopes and may be protective in vivo.Sci Transl Med. 2015 Apr 29;7(285):285ra63. doi: 10.1126/scitranslmed.aaa2546. Sci Transl Med. 2015. PMID: 25925682 Free PMC article.
-
A novel murine model of differentiation-mediated cytomegalovirus reactivation from latently infected bone marrow haematopoietic cells.J Gen Virol. 2019 Dec;100(12):1680-1694. doi: 10.1099/jgv.0.001327. J Gen Virol. 2019. PMID: 31647403 Free PMC article.
-
Immunotherapy for transplantation-associated viral infections.J Clin Invest. 2017 Jun 30;127(7):2513-2522. doi: 10.1172/JCI90599. Epub 2017 Jun 19. J Clin Invest. 2017. PMID: 28628043 Free PMC article. Review.
-
Limited Utility of Outpatient Surveillance Blood Cultures in Hematopoietic Cell Transplant Recipients on High-Dose Steroids for Treatment of Acute Graft-versus-Host-Disease.Biol Blood Marrow Transplant. 2019 Jun;25(6):1247-1252. doi: 10.1016/j.bbmt.2019.01.031. Epub 2019 Feb 1. Biol Blood Marrow Transplant. 2019. PMID: 30711778 Free PMC article.
References
-
- Boeckh M, Nichols WG. The impact of cytomegalovirus serostatus of donor and recipient before hematopoietic stem cell transplantation in the era of antiviral prophylaxis and preemptive therapy. Blood. 2004;103:2003–2008. - PubMed
-
- Nichols WG, Corey L, Gooley T, Davis C, Boeckh M. High risk of death due to bacterial and fungal infection among cytomegalovirus (CMV)-seronegative recipients of stem cell transplants from seropositive donors: evidence for indirect effects of primary CMV infection. J Infect Dis. 2002;185:273–282. - PubMed
-
- George B, Pati N, Gilroy N, et al. Pre-transplant cytomegalovirus (CMV) serostatus remains the most important determinant of CMV reactivation after allogeneic hematopoietic stem cell transplantation in the era of surveillance and preemptive therapy. Transpl Infect Dis. 2010;12:322–329. - PubMed
-
- Walker CM, van Burik JA, De For TE, Weisdorf DJ. Cytomegalovirus infection after allogeneic transplantation: comparison of cord blood with peripheral blood and marrow graft sources. Biol Blood Marrow Transplant. 2007;13:1106–1115. - PubMed
-
- Matthes-Martin S, Lion T, Aberle SW, et al. Pre-emptive treatment of CMV DNAemia in paediatric stem cell transplantation: the impact of recipient and donor CMV serostatus on the incidence of CMV disease and CMV-related mortality. Bone Marrow Transplant. 2003;31:803–808. - PubMed
