

Brain insulin resistance and deficiency as therapeutic targets in Alzheimer's disease
- PMID: 22329651
- PMCID: PMC3349985
- DOI: 10.2174/156720512799015037
Brain insulin resistance and deficiency as therapeutic targets in Alzheimer's disease
Abstract
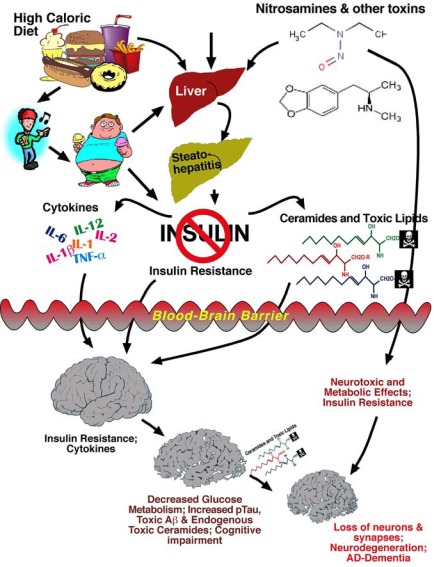
Alzheimer's disease [AD] is the most common cause of dementia in North America. Despite 30+ years of intense investigation, the field lacks consensus regarding the etiology and pathogenesis of sporadic AD, and therefore we still do not know the best strategies for treating and preventing this debilitating and costly disease. However, growing evidence supports the concept that AD is fundamentally a metabolic disease with substantial and progressive derangements in brain glucose utilization and responsiveness to insulin and insulin-like growth factor [IGF] stimulation. Moreover, AD is now recognized to be heterogeneous in nature, and not solely the end-product of aberrantly processed, misfolded, and aggregated oligomeric amyloid-beta peptides and hyperphosphorylated tau. Other factors, including impairments in energy metabolism, increased oxidative stress, inflammation, insulin and IGF resistance, and insulin/IGF deficiency in the brain should be incorporated into all equations used to develop diagnostic and therapeutic approaches to AD. Herein, the contributions of impaired insulin and IGF signaling to AD-associated neuronal loss, synaptic disconnection, tau hyperphosphorylation, amyloid-beta accumulation, and impaired energy metabolism are reviewed. In addition, we discuss current therapeutic strategies and suggest additional approaches based on the hypothesis that AD is principally a metabolic disease similar to diabetes mellitus. Ultimately, our ability to effectively detect, monitor, treat, and prevent AD will require more efficient, accurate and integrative diagnostic tools that utilize clinical, neuroimaging, biochemical, and molecular biomarker data. Finally, it is imperative that future therapeutic strategies for AD abandon the concept of uni-modal therapy in favor of multi-modal treatments that target distinct impairments at different levels within the brain insulin/IGF signaling cascades.
Figures


Similar articles
-
Contributions of brain insulin resistance and deficiency in amyloid-related neurodegeneration in Alzheimer's disease.Drugs. 2012 Jan 1;72(1):49-66. doi: 10.2165/11597760-000000000-00000. Drugs. 2012. PMID: 22191795 Free PMC article. Review.
-
Therapeutic targets of brain insulin resistance in sporadic Alzheimer's disease.Front Biosci (Elite Ed). 2012 Jan 1;4(4):1582-605. doi: 10.2741/e482. Front Biosci (Elite Ed). 2012. PMID: 22201977 Free PMC article. Review.
-
Type 3 diabetes is sporadic Alzheimer׳s disease: mini-review.Eur Neuropsychopharmacol. 2014 Dec;24(12):1954-60. doi: 10.1016/j.euroneuro.2014.06.008. Epub 2014 Jun 28. Eur Neuropsychopharmacol. 2014. PMID: 25088942 Free PMC article. Review.
-
Decoding Alzheimer's disease from perturbed cerebral glucose metabolism: implications for diagnostic and therapeutic strategies.Prog Neurobiol. 2013 Sep;108:21-43. doi: 10.1016/j.pneurobio.2013.06.004. Epub 2013 Jul 11. Prog Neurobiol. 2013. PMID: 23850509 Review.
-
Conquering Insulin Network Dysfunctions in Alzheimer's Disease: Where Are We Today?J Alzheimers Dis. 2024;101(s1):S317-S343. doi: 10.3233/JAD-240069. J Alzheimers Dis. 2024. PMID: 39422949 Review.
Cited by
-
Resveratrol supplementation confers neuroprotection in cortical brain tissue of nonhuman primates fed a high-fat/sucrose diet.Aging (Albany NY). 2016 May;8(5):899-916. doi: 10.18632/aging.100942. Aging (Albany NY). 2016. PMID: 27070252 Free PMC article.
-
The Role of the Neural Exposome as a Novel Strategy to Identify and Mitigate Health Inequities in Alzheimer's Disease and Related Dementias.Mol Neurobiol. 2025 Jan;62(1):1205-1224. doi: 10.1007/s12035-024-04339-6. Epub 2024 Jul 5. Mol Neurobiol. 2025. PMID: 38967905 Free PMC article. Review.
-
Central Regulation of Glucose Production May Be Impaired in Type 2 Diabetes.Diabetes. 2016 Sep;65(9):2569-79. doi: 10.2337/db15-1465. Epub 2016 May 10. Diabetes. 2016. PMID: 27207526 Free PMC article. Clinical Trial.
-
Type 2 Diabetes Mellitus and Alzheimer's Disease: Shared Molecular Mechanisms and Potential Common Therapeutic Targets.Int J Mol Sci. 2022 Dec 4;23(23):15287. doi: 10.3390/ijms232315287. Int J Mol Sci. 2022. PMID: 36499613 Free PMC article. Review.
-
Early-Stage Alzheimer's Disease Is Associated with Simultaneous Systemic and Central Nervous System Dysregulation of Insulin-Linked Metabolic Pathways.J Alzheimers Dis. 2019;68(2):657-668. doi: 10.3233/JAD-180906. J Alzheimers Dis. 2019. PMID: 30775986 Free PMC article.
References
-
- Cummings JL. In: Definitions and diagnostic criteria. Third ed. Gauthier S, editor. London: Informa UK Limited; 2007.
-
- Frolich L, Blum-Degen D, Bernstein HG, Engelsberger S, Humrich J, Laufer S, et al. Brain insulin and insulin receptors in aging and sporadic Alzheimer's disease. J Neural Transm. 1998;105(4-5):423–438. - PubMed
-
- Hoyer S. The brain insulin signal transduction system and sporadic (type II) Alzheimer disease: an update. J Neural Transm. 2002;109(3):341–360. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical