

Generation of polyclonal CMV-specific T cells for the adoptive immunotherapy of glioblastoma
- PMID: 22306904
- PMCID: PMC3280423
- DOI: 10.1097/CJI.0b013e318247642f
Generation of polyclonal CMV-specific T cells for the adoptive immunotherapy of glioblastoma
Abstract
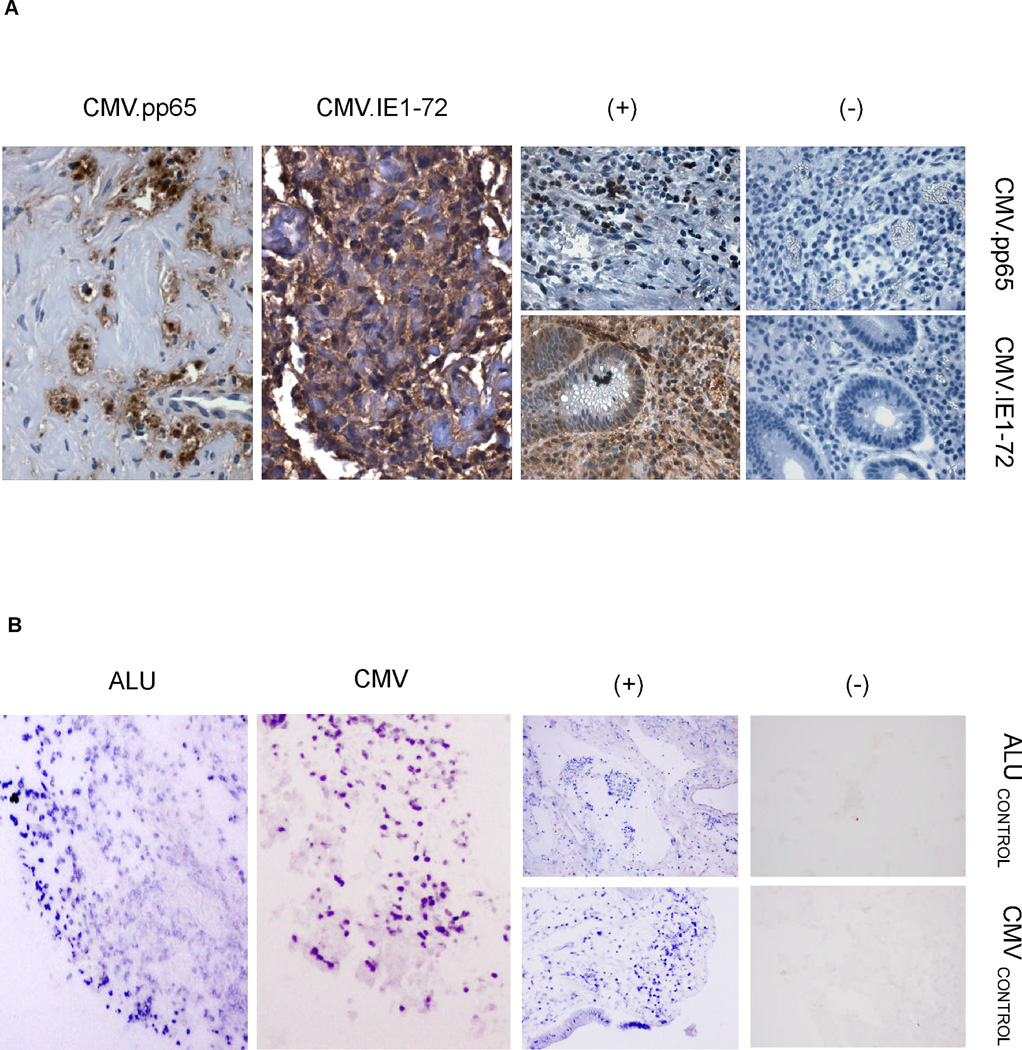
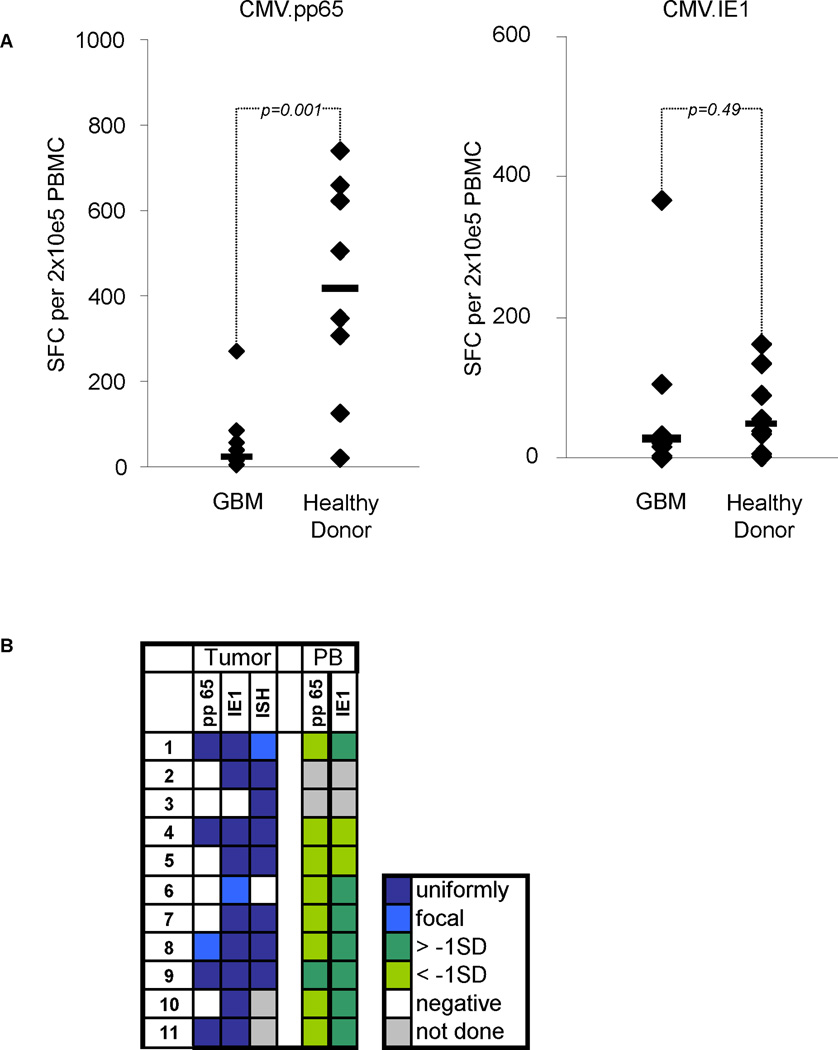
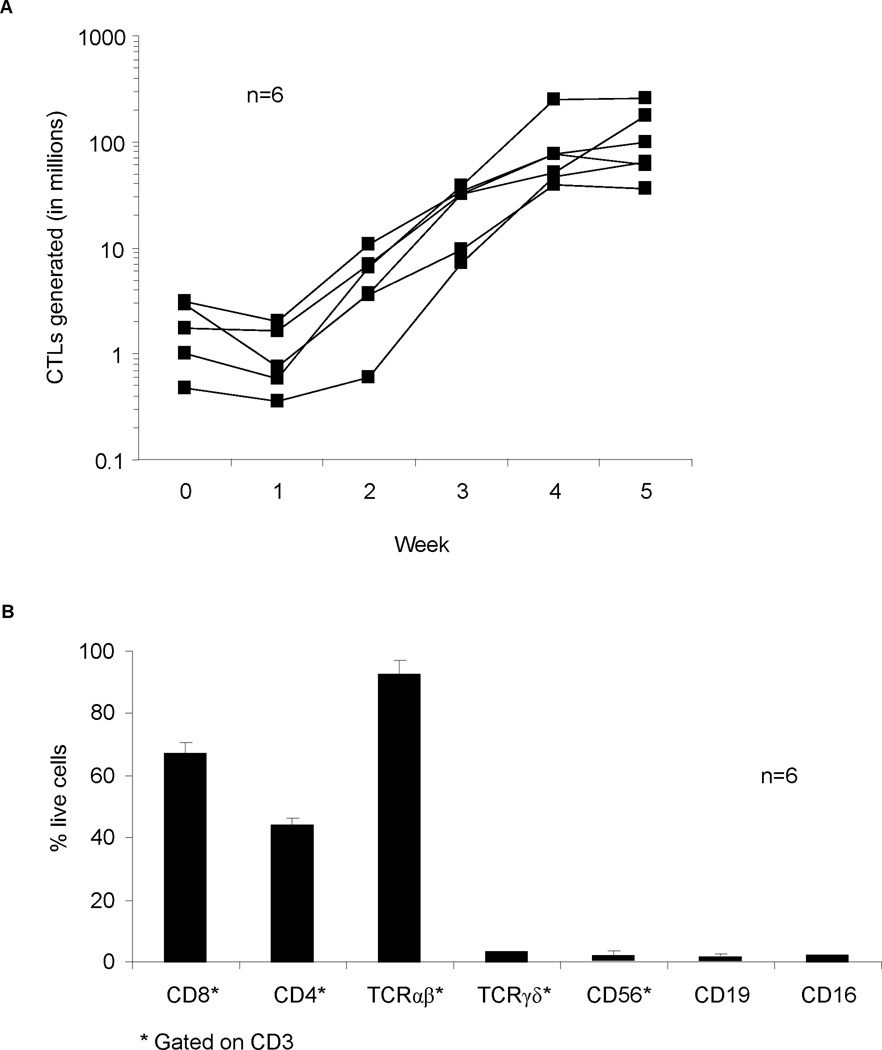
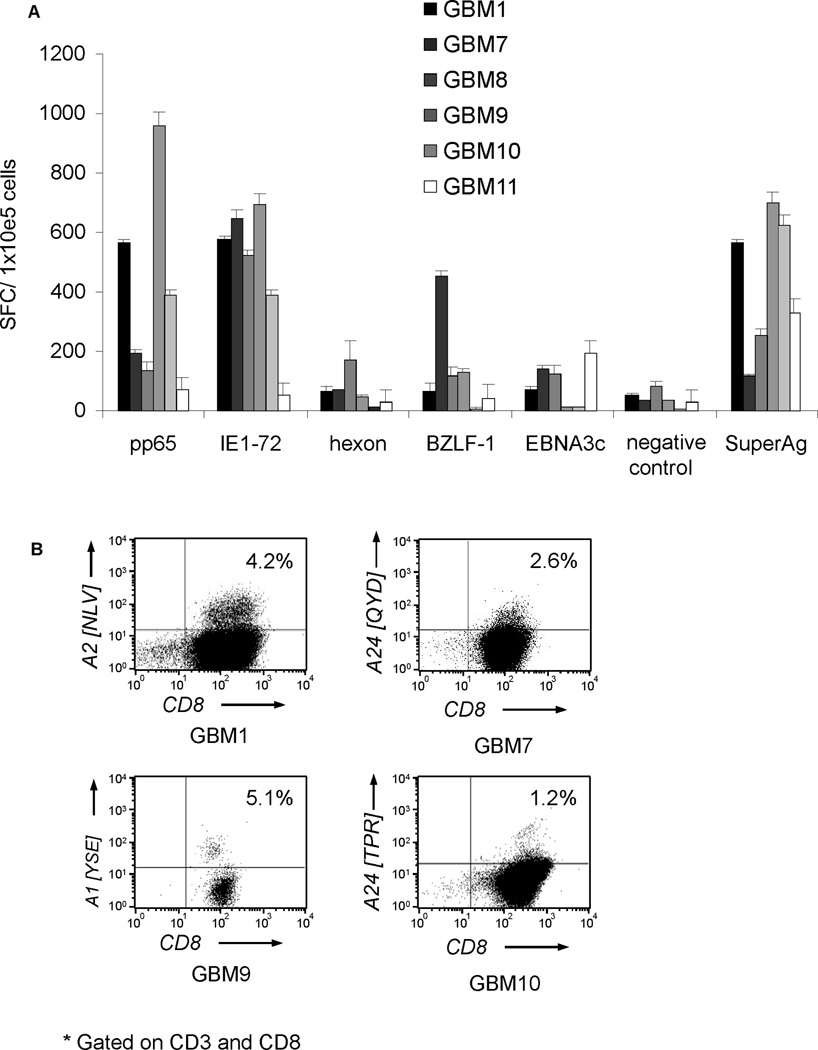
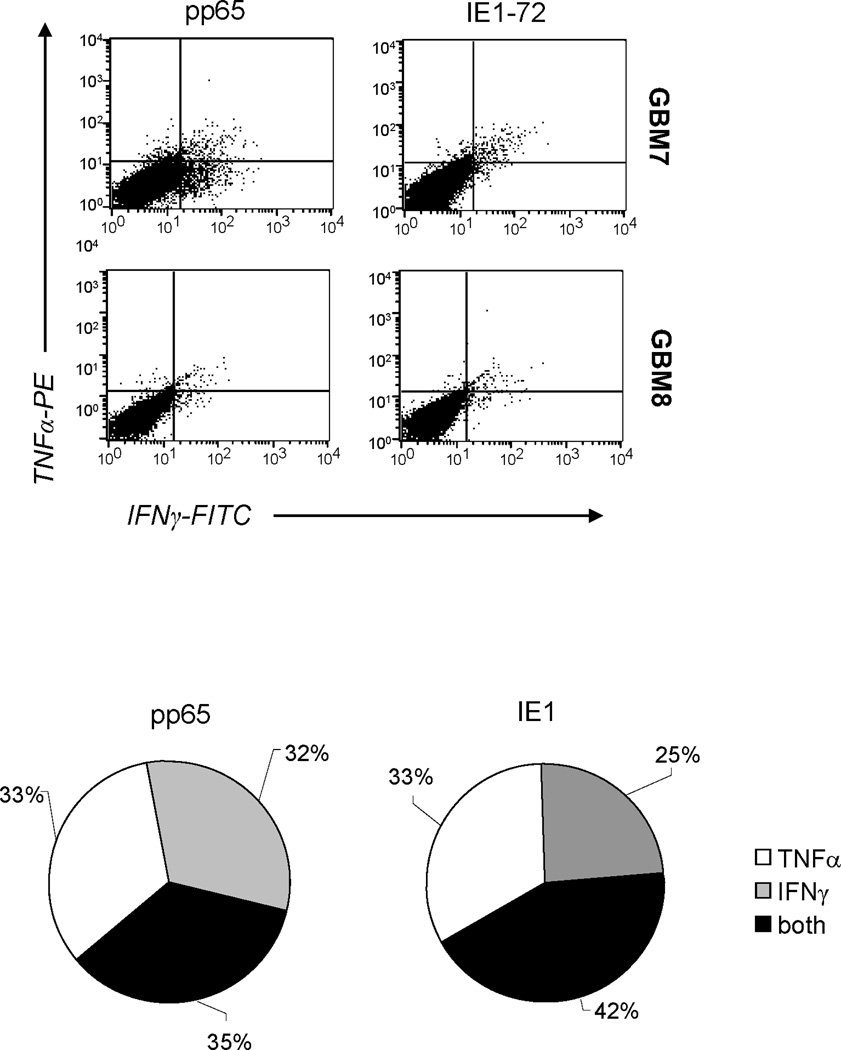
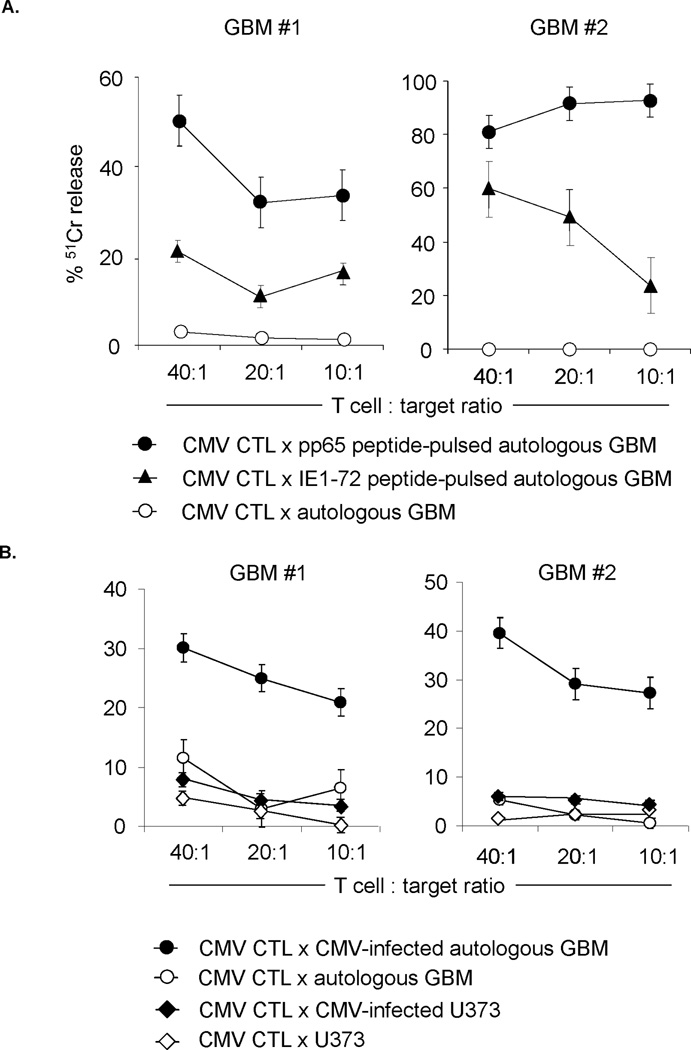
Glioblastoma (GBM) is the most common primary brain cancer in adults and is virtually incurable. Recent studies have shown that cytomegalovirus (CMV) is present in majority of GBMs. To evaluate whether the CMV antigens pp65 and IE1, which are expressed in GBMs, could be targeted by CMV-specific T cells, we measured the frequency of T cells targeting pp65 and IE1 in the peripheral blood of a cohort of 11 sequentially diagnosed CMV-seropositive GBM patients, and evaluated whether it was feasible to expand autologous CMV-specific T cells for future clinical studies. All 11 CMV-seropositive GBM patients had T cells specific for pp65 and IE1 in their peripheral blood assessed by IFNγ enzyme-linked immunospot assay. However, the precursor frequency of pp65-specific T cells was decreased in comparison with healthy donors (P=0.001). We successfully reactivated and expanded CMV-specific T cells from 6 out of 6 GBM patients using antigen-presenting cells transduced with an adenoviral vector encoding pp65 and IE1. CMV-specific T-cell lines contained CD4 as well as CD8 T cells, recognized pp65 and IE1 targets and killed CMV-infected autologous GBM cells. Infusion of such CMV-specific T-cell lines may extend the benefits of T-cell therapy to patients with CMV GBMs.
Conflict of interest statement
Figures
Similar articles
-
The detection of CMV pp65 and IE1 in glioblastoma multiforme.J Neurooncol. 2011 Jun;103(2):231-8. doi: 10.1007/s11060-010-0383-6. Epub 2010 Sep 5. J Neurooncol. 2011. PMID: 20820869
-
Dendritic Cells Enhance Polyfunctionality of Adoptively Transferred T Cells That Target Cytomegalovirus in Glioblastoma.Cancer Res. 2018 Jan 1;78(1):256-264. doi: 10.1158/0008-5472.CAN-17-0469. Epub 2017 Nov 1. Cancer Res. 2018. PMID: 29093005 Free PMC article. Clinical Trial.
-
Recognition and killing of autologous, primary glioblastoma tumor cells by human cytomegalovirus pp65-specific cytotoxic T cells.Clin Cancer Res. 2014 May 15;20(10):2684-94. doi: 10.1158/1078-0432.CCR-13-3268. Epub 2014 Mar 21. Clin Cancer Res. 2014. PMID: 24658154 Free PMC article.
-
Cytomegalovirus-targeted immunotherapy and glioblastoma: hype or hope?Immunotherapy. 2016;8(4):413-23. doi: 10.2217/imt.16.2. Immunotherapy. 2016. PMID: 26973123 Review.
-
Refining human T-cell immunotherapy of cytomegalovirus disease: a mouse model with 'humanized' antigen presentation as a new preclinical study tool.Med Microbiol Immunol. 2016 Dec;205(6):549-561. doi: 10.1007/s00430-016-0471-0. Epub 2016 Aug 18. Med Microbiol Immunol. 2016. PMID: 27539576 Review.
Cited by
-
Human cytomegalovirus seropositivity is associated with decreased survival in glioblastoma patients.Neurooncol Adv. 2019 Sep 7;1(1):vdz020. doi: 10.1093/noajnl/vdz020. eCollection 2019 May-Dec. Neurooncol Adv. 2019. PMID: 32642656 Free PMC article.
-
Novel Pharmacological Treatment Options in Pediatric Glioblastoma-A Systematic Review.Cancers (Basel). 2022 Jun 6;14(11):2814. doi: 10.3390/cancers14112814. Cancers (Basel). 2022. PMID: 35681794 Free PMC article. Review.
-
New extracellular factors in glioblastoma multiforme development: neurotensin, growth differentiation factor-15, sphingosine-1-phosphate and cytomegalovirus infection.Oncotarget. 2018 Jan 9;9(6):7219-7270. doi: 10.18632/oncotarget.24102. eCollection 2018 Jan 23. Oncotarget. 2018. PMID: 29467963 Free PMC article. Review.
-
Presence of the Human Cytomegalovirus in Glioblastomas-A Systematic Review.Cancers (Basel). 2021 Oct 9;13(20):5051. doi: 10.3390/cancers13205051. Cancers (Basel). 2021. PMID: 34680198 Free PMC article. Review.
-
A new hope in immunotherapy for malignant gliomas: adoptive T cell transfer therapy.J Immunol Res. 2014;2014:326545. doi: 10.1155/2014/326545. Epub 2014 Jun 9. J Immunol Res. 2014. PMID: 25009822 Free PMC article. Review.
References
-
- Buckner JC. Factors influencing survival in high-grade gliomas. Semin Oncol. 2003;30:10–14. - PubMed
-
- Stupp R, Mason WP, Van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–996. - PubMed
-
- DeAngelis LM. Brain tumors. N Engl J Med. 2001;344:114–123. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
