

Increased intratumoral neutrophil in colorectal carcinomas correlates closely with malignant phenotype and predicts patients' adverse prognosis
- PMID: 22295111
- PMCID: PMC3266280
- DOI: 10.1371/journal.pone.0030806
Increased intratumoral neutrophil in colorectal carcinomas correlates closely with malignant phenotype and predicts patients' adverse prognosis
Abstract
Background: Substantial evidence suggests that the presence of inflammatory cells plays a critical role in the development and/or progression of human tumors. Neutrophils are the common inflammatory cells in tumors; however, the infiltration of intratumoral neutrophils in colorectal carcinoma (CRC) and its effect on CRC patients' prognosis are poorly understood.
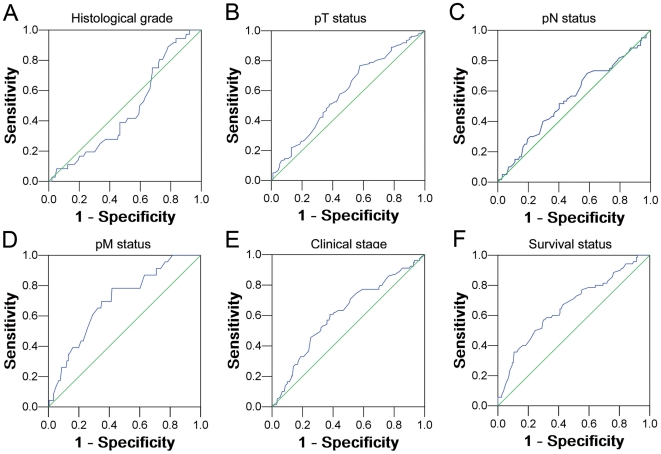
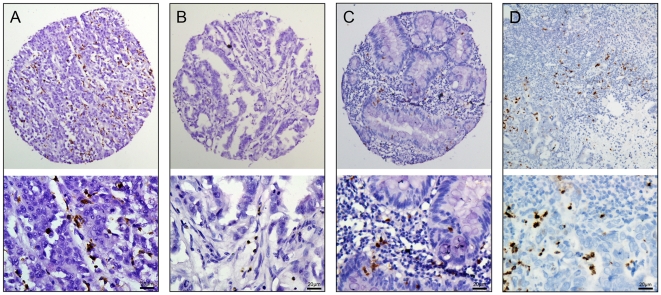
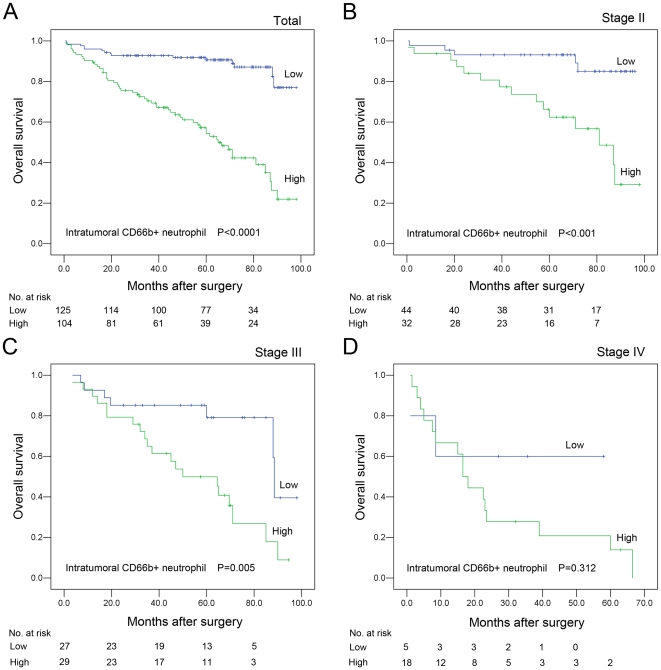
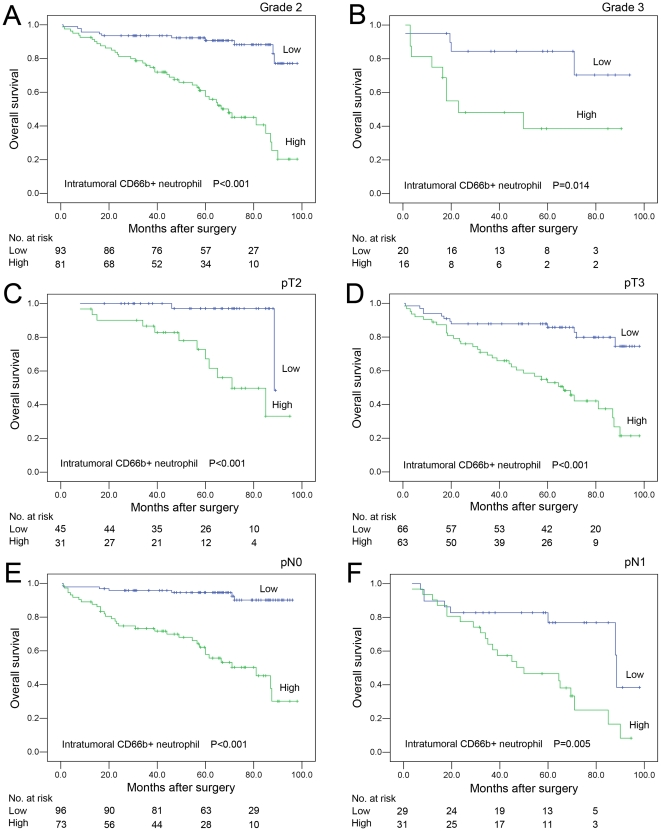
Methodology/principal findings: In this study, the methods of tissue microarray and immunohistochemistry (IHC) were used to investigate the prognostic significance of intratumoral CD66b+ neutrophil in CRC. According to receiver operating characteristic curve analysis, the cutoff score for high intratumoral CD66b+ neutrophil in CRC was defined when the mean counts were more than 60 per TMA spot. In our study, high intratumoral CD66b+ neutrophil was observed in 104/229 (45.4%) of CRCs and in 29/229 (12.7%) of adjacent mucosal tissues. Further correlation analysis showed that high intratumoral neutrophil was positively correlated with pT status, pM status and clinical stage (P<0.05). In univariate survival analysis, a significant association between high intratumoral neutrophil and shortened patients' survival was found (P<0.0001). In different subsets of CRC patients, intratumoral neutrophil was also a prognostic indicator in patients with stage II, stage III, grade 2, grade 3, pT1, pT2, pN0 and pN1 (P<0.05). Importantly, high intratumoral neutrophil was evaluated as an independent prognostic factor in multivariate analysis (P<0.05).
Conclusions/significance: Our results provide evidence that increased intratumoral neutrophil in CRC may be important in the acquisition of a malignant phenotype, indicating that the presence of intratumoral neutrophil is an independent factor for poor prognosis of patients with CRC.
Conflict of interest statement
Figures
Similar articles
-
Neutrophil infiltration is a favorable prognostic factor in early stages of colon cancer.Hum Pathol. 2017 Oct;68:193-202. doi: 10.1016/j.humpath.2017.08.028. Epub 2017 Sep 4. Hum Pathol. 2017. PMID: 28882699
-
High myeloperoxidase positive cell infiltration in colorectal cancer is an independent favorable prognostic factor.PLoS One. 2013 May 29;8(5):e64814. doi: 10.1371/journal.pone.0064814. Print 2013. PLoS One. 2013. PMID: 23734221 Free PMC article.
-
Intratumoral neutrophils: a poor prognostic factor for hepatocellular carcinoma following resection.J Hepatol. 2011 Mar;54(3):497-505. doi: 10.1016/j.jhep.2010.07.044. Epub 2010 Oct 1. J Hepatol. 2011. PMID: 21112656
-
Prognostic effect of intratumoral neutrophils across histological subtypes of non-small cell lung cancer.Oncotarget. 2016 Nov 1;7(44):72184-72196. doi: 10.18632/oncotarget.12360. Oncotarget. 2016. PMID: 27708229 Free PMC article.
-
Tumor-associated neutrophils as a new prognostic factor in cancer: a systematic review and meta-analysis.PLoS One. 2014 Jun 6;9(6):e98259. doi: 10.1371/journal.pone.0098259. eCollection 2014. PLoS One. 2014. PMID: 24906014 Free PMC article. Review.
Cited by
-
Neutrophils promote tumor resistance to radiation therapy.Proc Natl Acad Sci U S A. 2019 Sep 10;116(37):18584-18589. doi: 10.1073/pnas.1901562116. Epub 2019 Aug 28. Proc Natl Acad Sci U S A. 2019. PMID: 31462499 Free PMC article.
-
Integrative analysis identifies DNMTs against immune-infiltrating neutrophils and dendritic cells in colorectal cancer.Epigenetics. 2019 Apr;14(4):392-404. doi: 10.1080/15592294.2019.1588684. Epub 2019 Mar 16. Epigenetics. 2019. PMID: 30880552 Free PMC article.
-
Prognostic significance of inflammatory cell response in patients with colorectal cancer.Oncol Lett. 2019 Jul;18(1):783-791. doi: 10.3892/ol.2019.10343. Epub 2019 May 13. Oncol Lett. 2019. PMID: 31289555 Free PMC article.
-
Contribution to Tumor Angiogenesis From Innate Immune Cells Within the Tumor Microenvironment: Implications for Immunotherapy.Front Immunol. 2018 Apr 5;9:527. doi: 10.3389/fimmu.2018.00527. eCollection 2018. Front Immunol. 2018. PMID: 29675018 Free PMC article. Review.
-
Mathematical prediction of clinical outcomes in advanced cancer patients treated with checkpoint inhibitor immunotherapy.Sci Adv. 2020 Apr 29;6(18):eaay6298. doi: 10.1126/sciadv.aay6298. eCollection 2020 May. Sci Adv. 2020. PMID: 32426472 Free PMC article.
References
-
- O'Connell JB, Maggard MA, Ko CY. Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J Natl Cancer Inst. 2004;96:1420–1425. - PubMed
-
- You WC, Jin F, Devesa S, Gridley G, Schatzkin A, et al. Rapid increase in colorectal cancer rates in urban Shanghai, 1972–97, in relation to dietary changes. J Cancer Epidemiol Prev. 2002;7:143–146. - PubMed
-
- Obrand DI, Gordon PH. Incidence and patterns of recurrence following curative resection for colorectal carcinoma. Dis Colon Rectum. 1997;40:15–24. - PubMed
-
- Zafirellis K, Agrogiannis G, Zachaki A, Gravani K, Karameris A, et al. Prognostic significance of VEGF expression evaluated by quantitative immunohistochemical analysis in colorectal cancer. J Surg Res. 2008;147:99–107. - PubMed
-
- Mantovani A. Cancer: Inflaming metastasis. Nature. 2009;457:36–37. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
