

Absence of SOCS3 in the cardiomyocyte increases mortality in a gp130-dependent manner accompanied by contractile dysfunction and ventricular arrhythmias
- PMID: 22082679
- PMCID: PMC3253669
- DOI: 10.1161/CIRCULATIONAHA.111.028498
Absence of SOCS3 in the cardiomyocyte increases mortality in a gp130-dependent manner accompanied by contractile dysfunction and ventricular arrhythmias
Abstract
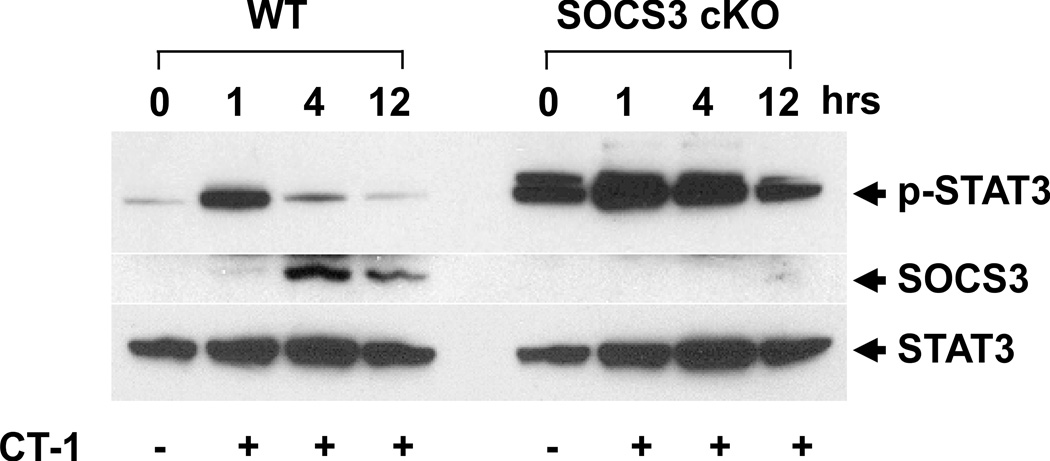
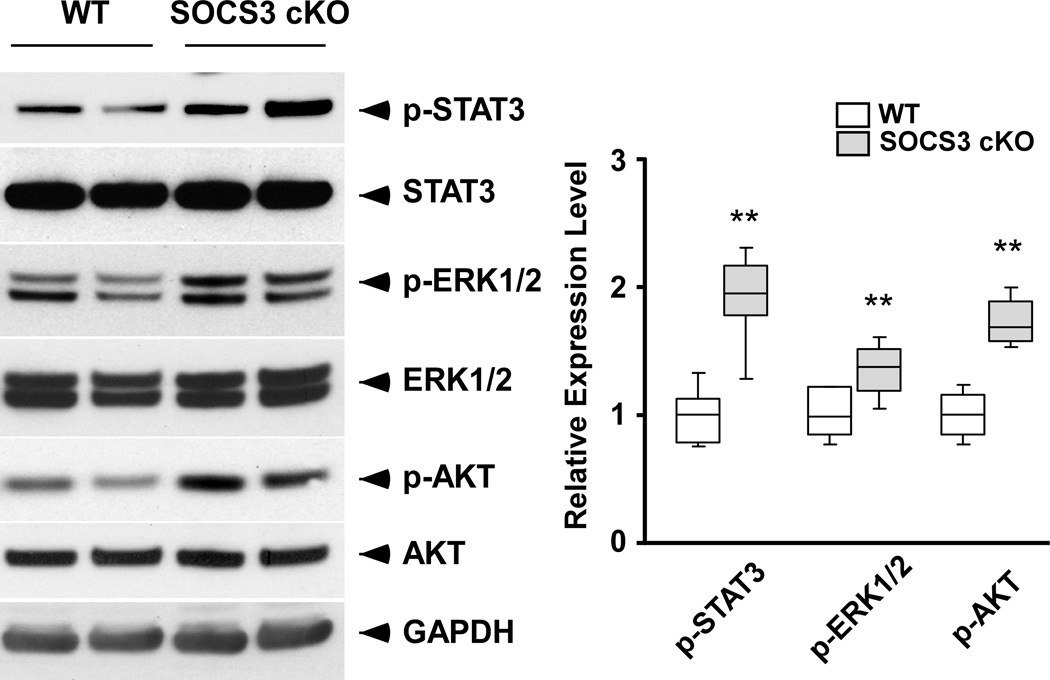
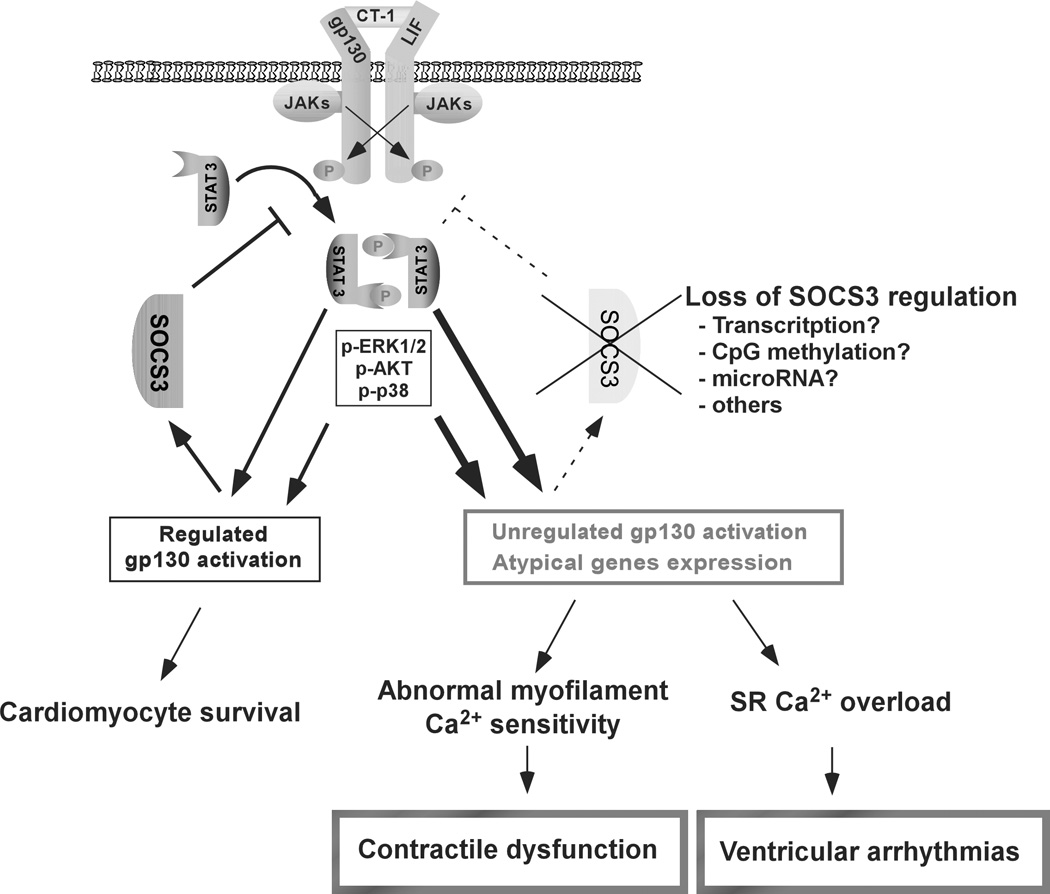
Background: Suppressor of cytokine signaling-3 (SOCS3) is a key negative-feedback regulator of the gp130 receptor that provides crucial signaling for cardiac hypertrophy and survival; however, an in vivo role of SOCS3 regulation on cardiac gp130 signaling remains obscure.
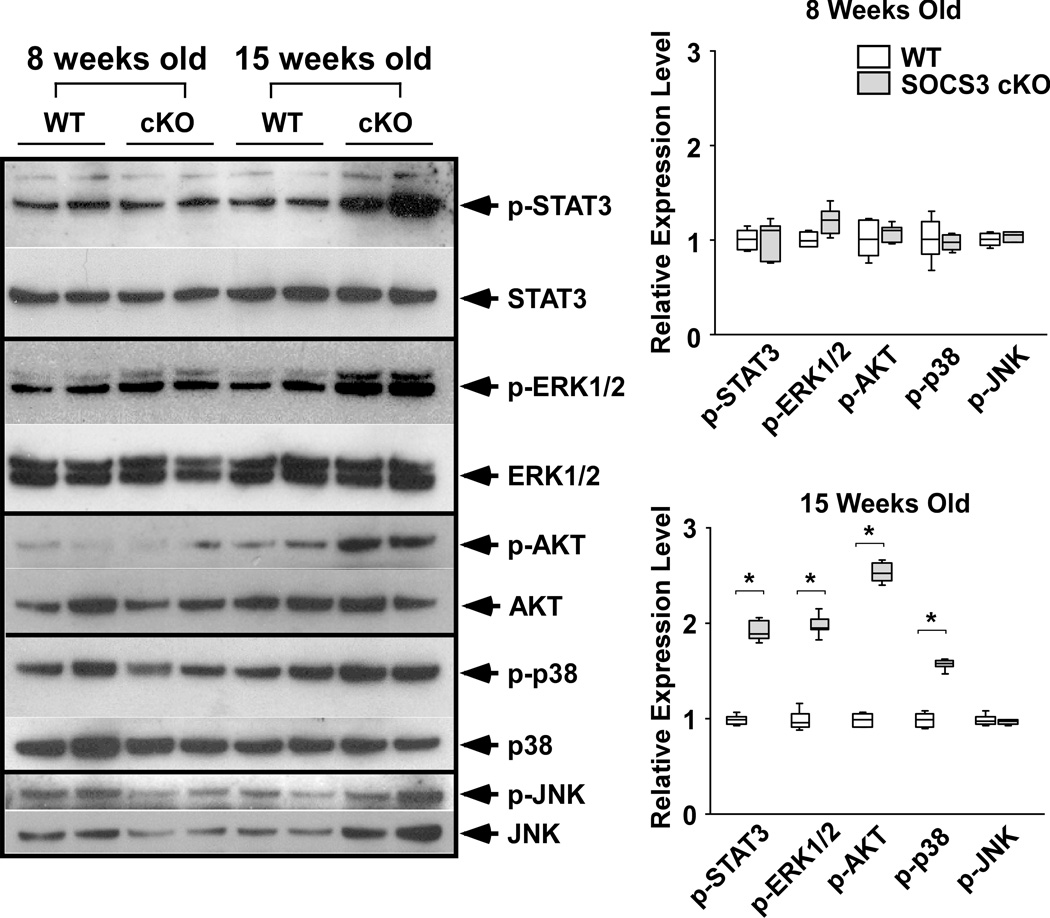
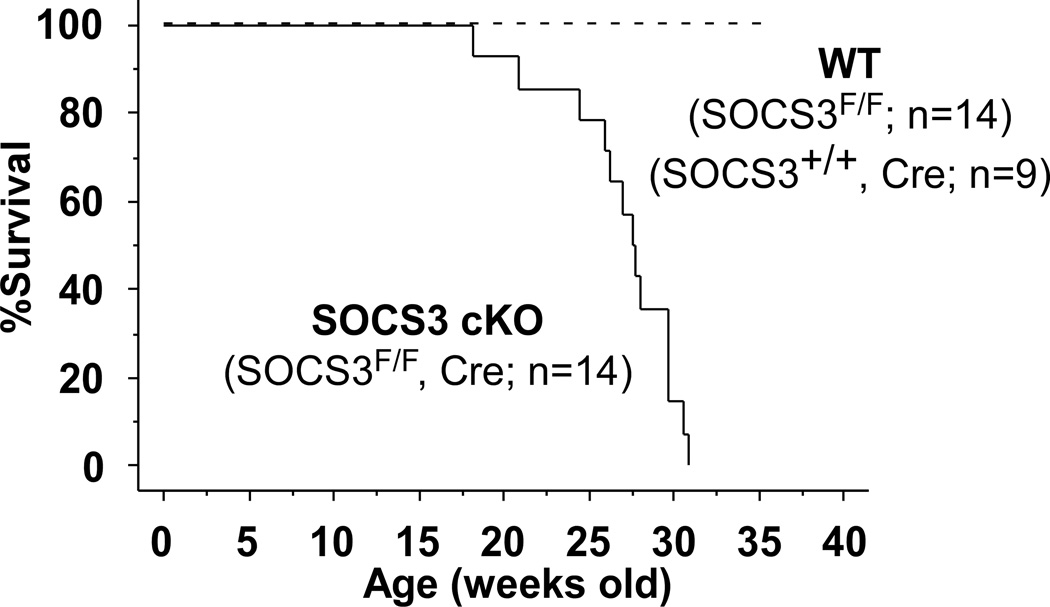
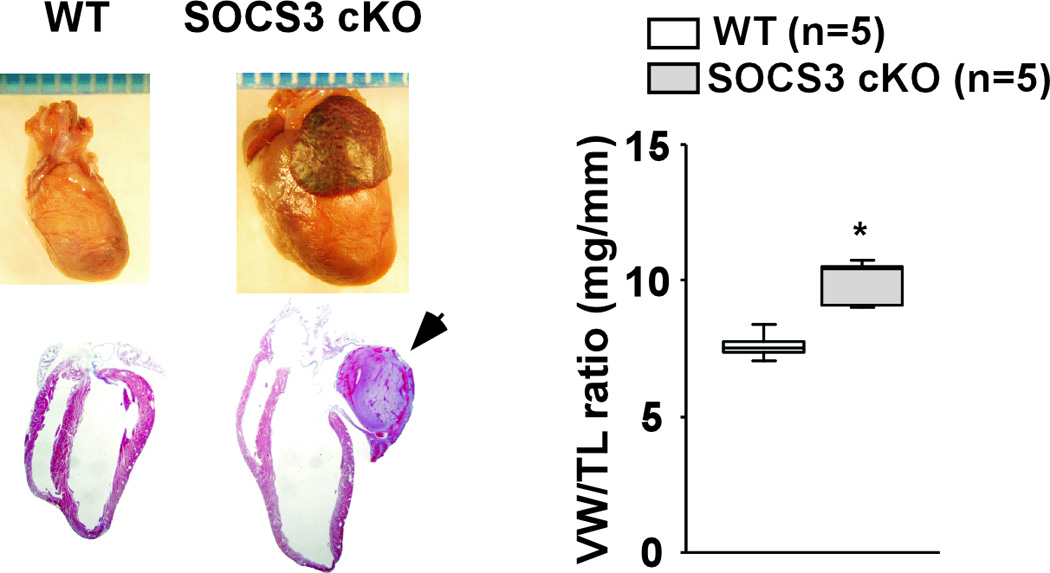
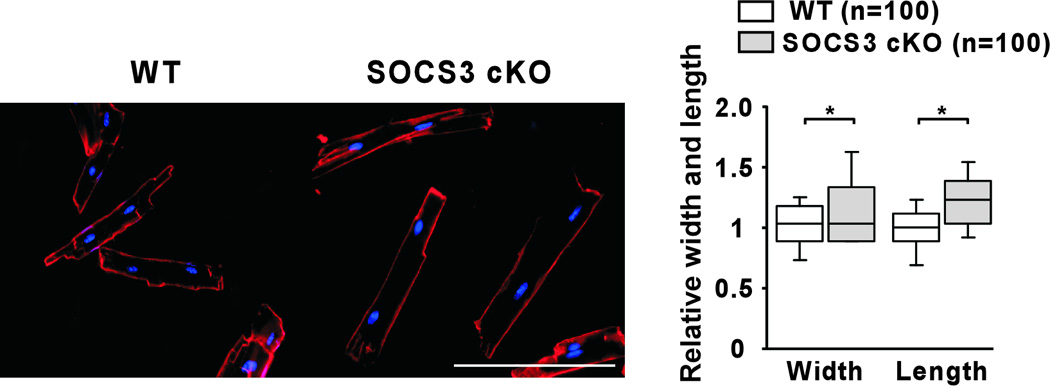
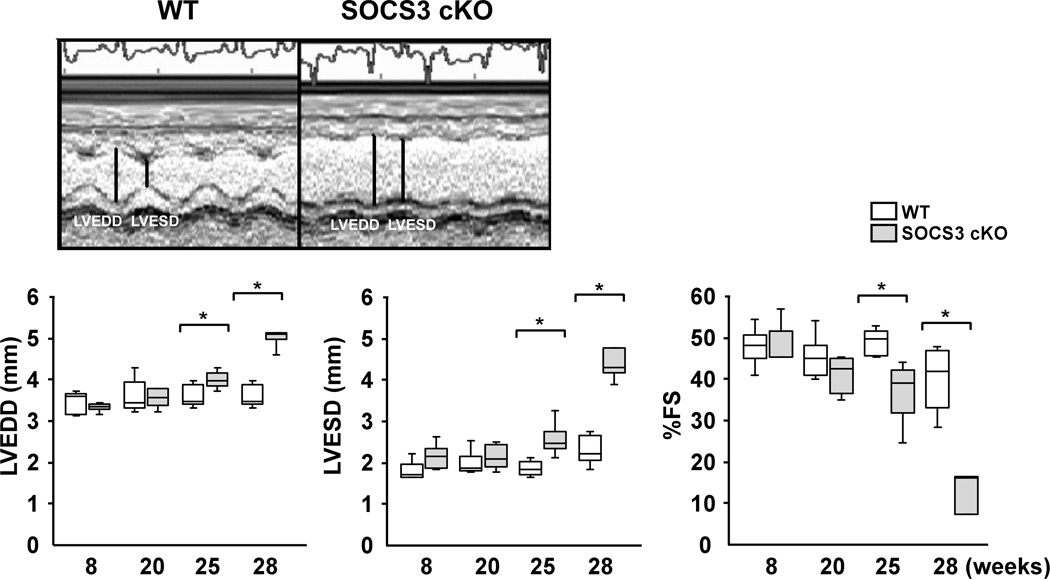
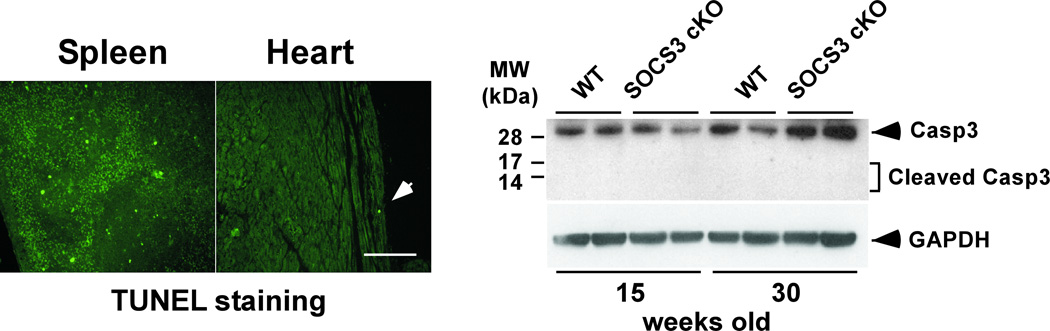
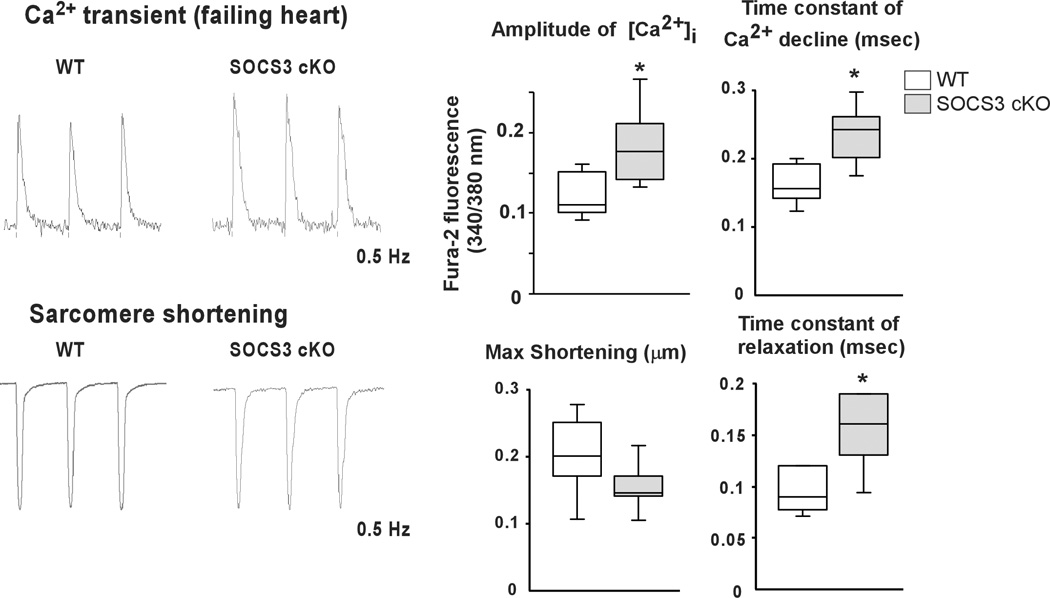
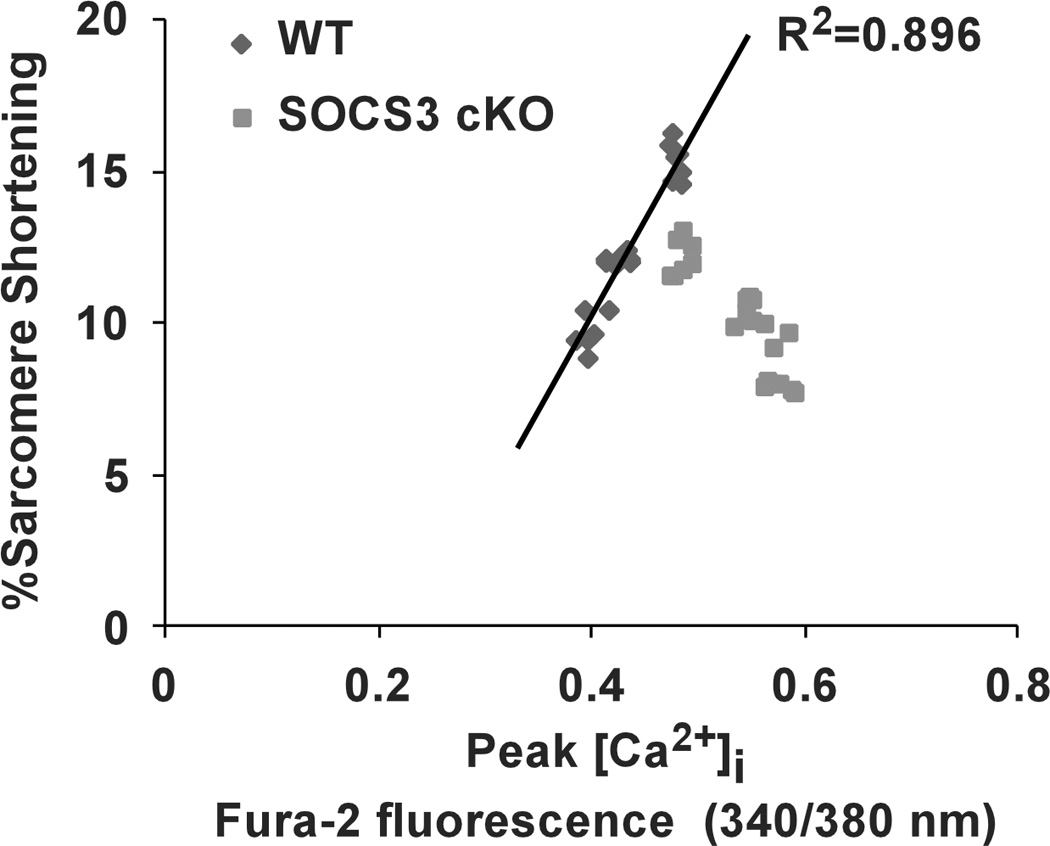
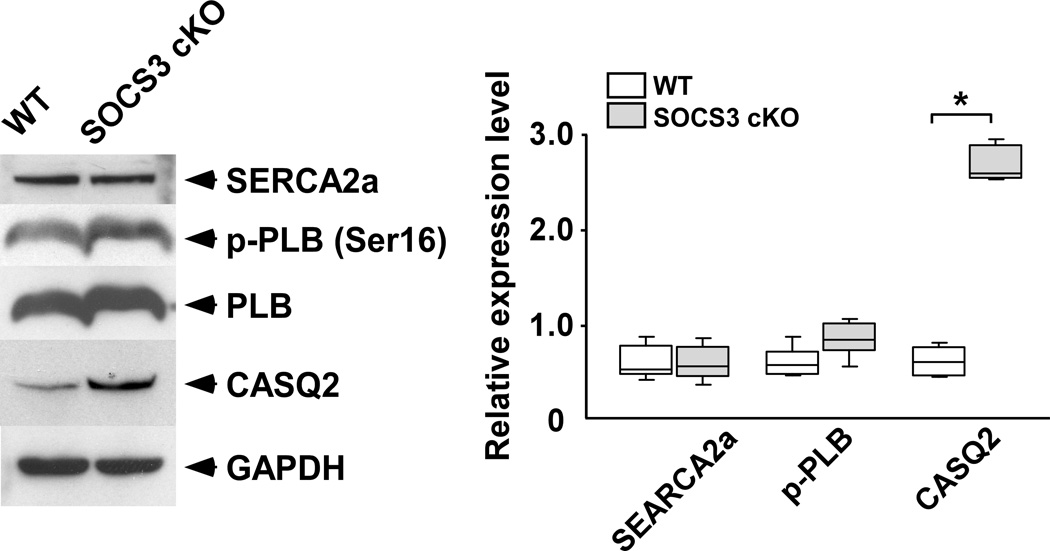
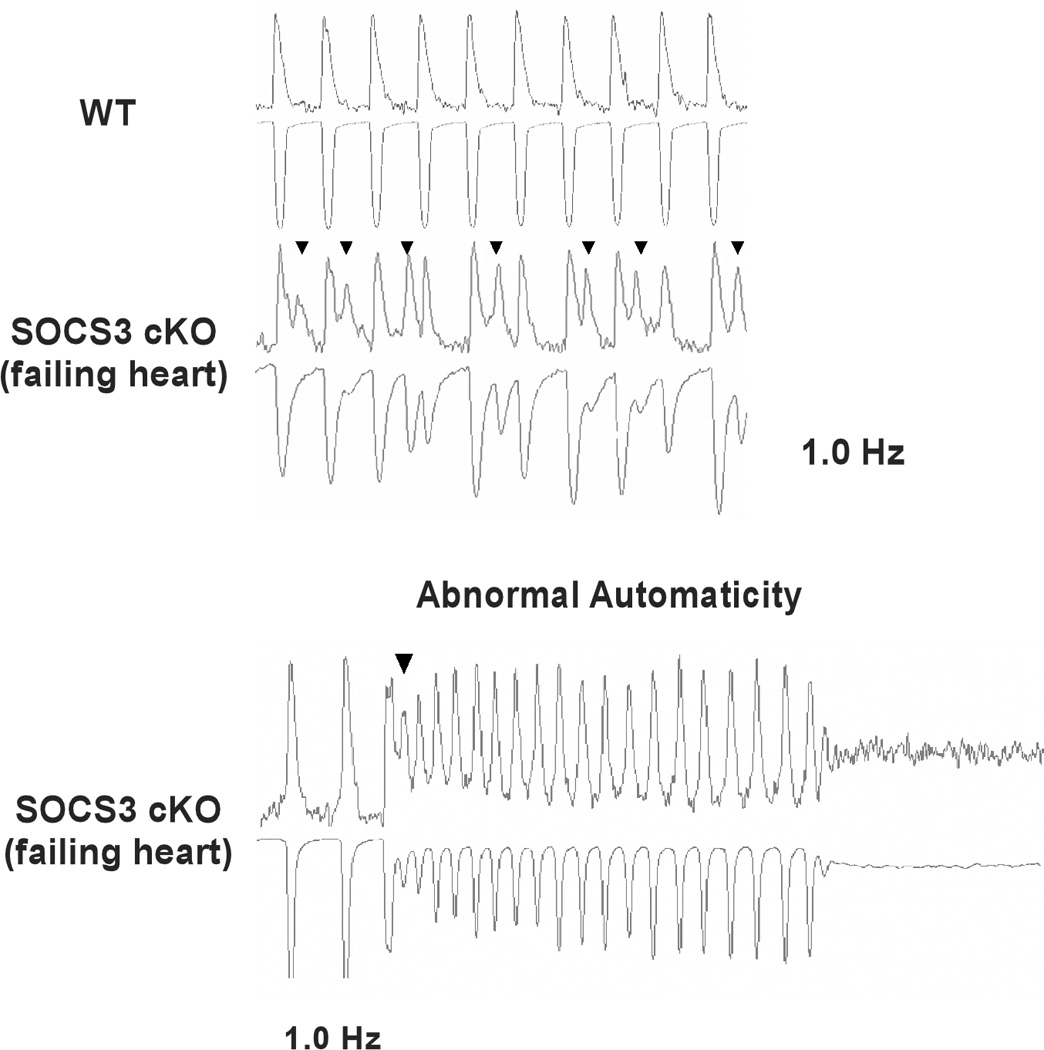
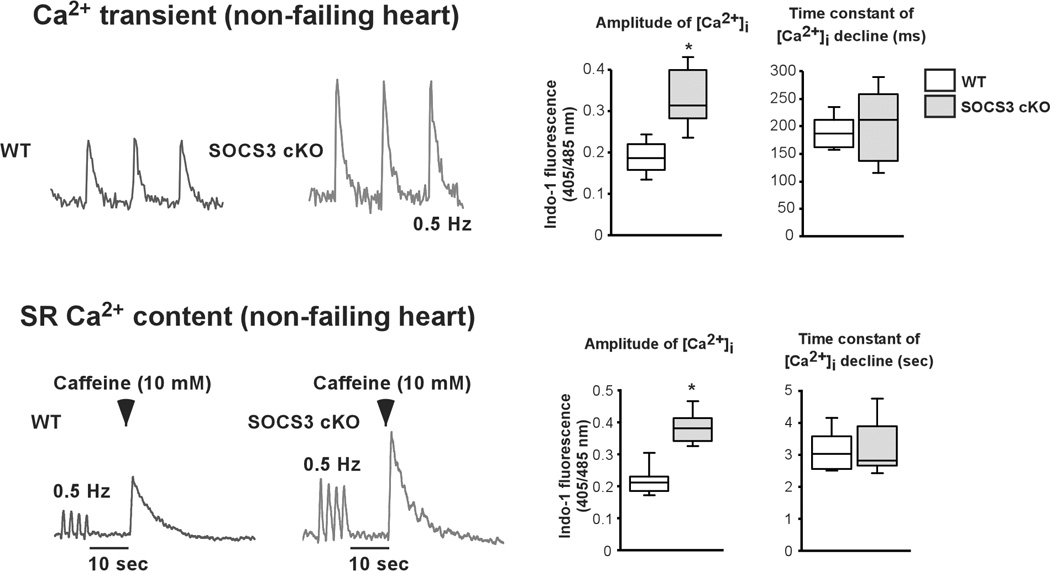
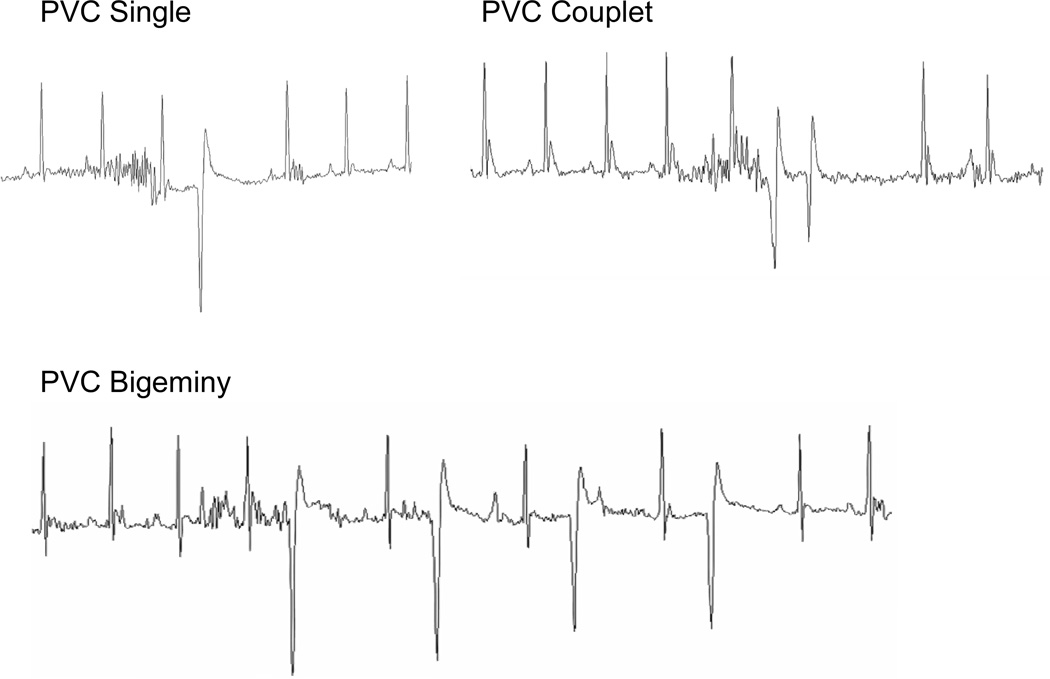
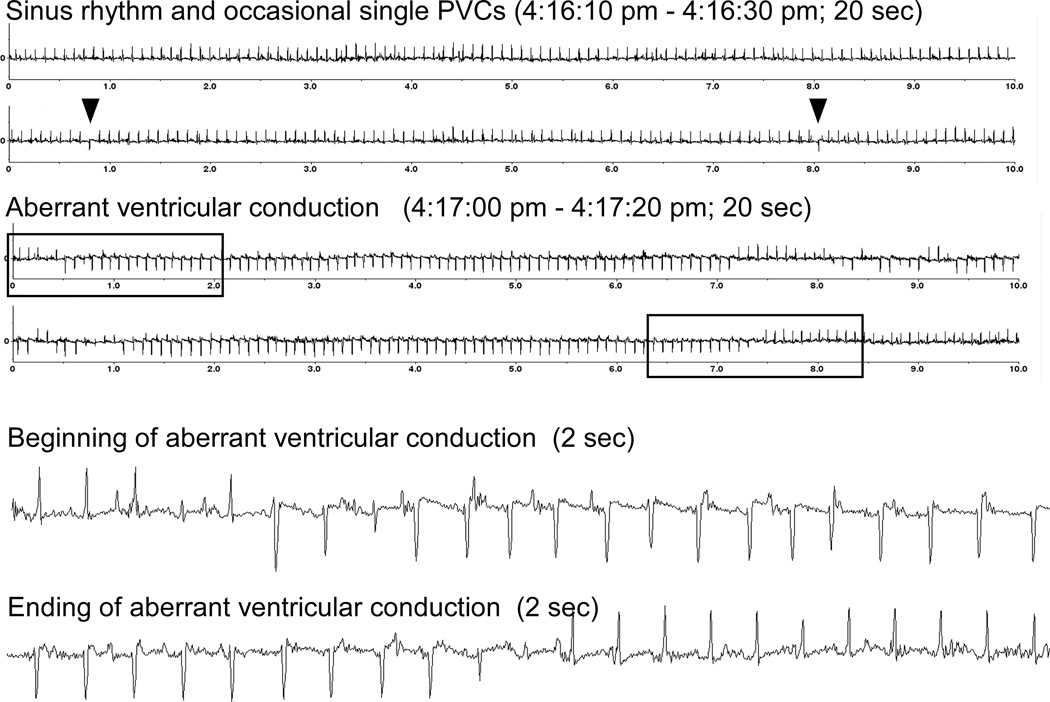
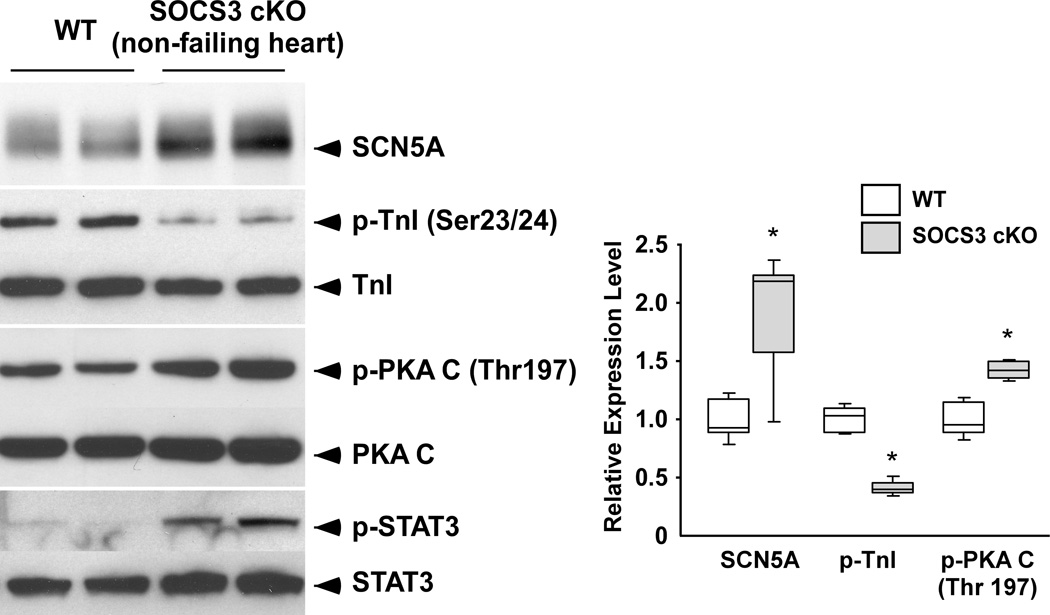
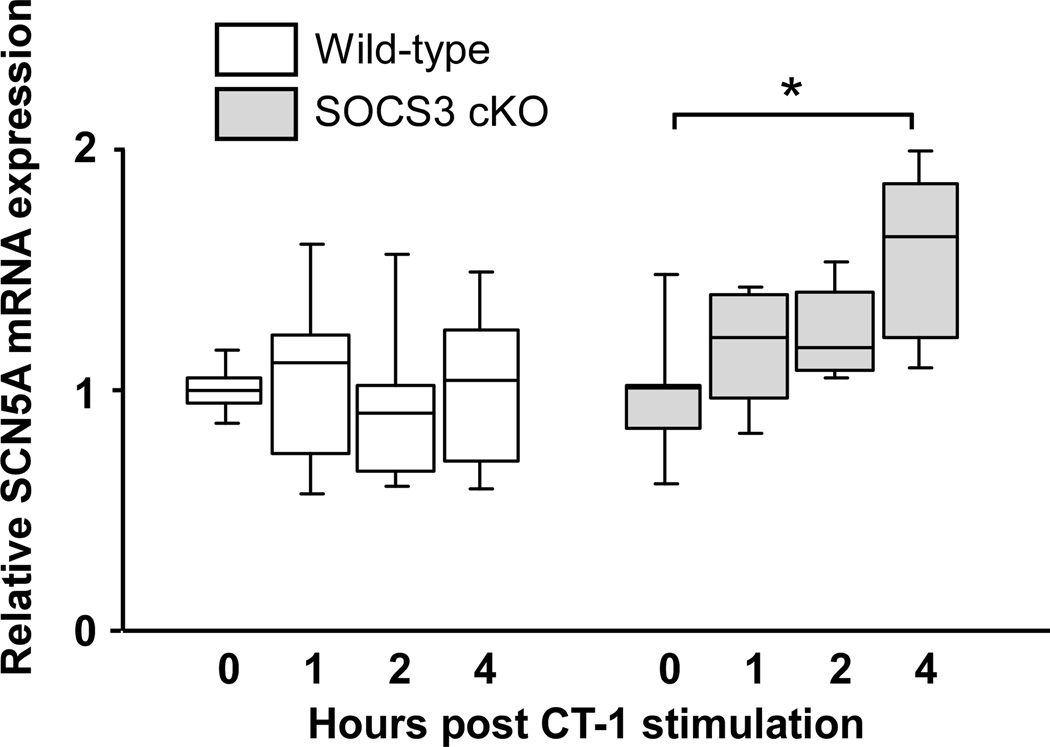
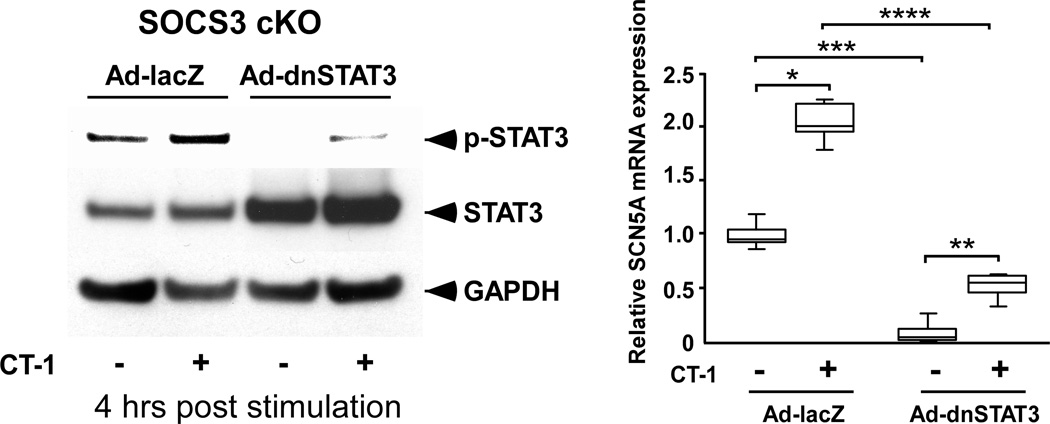
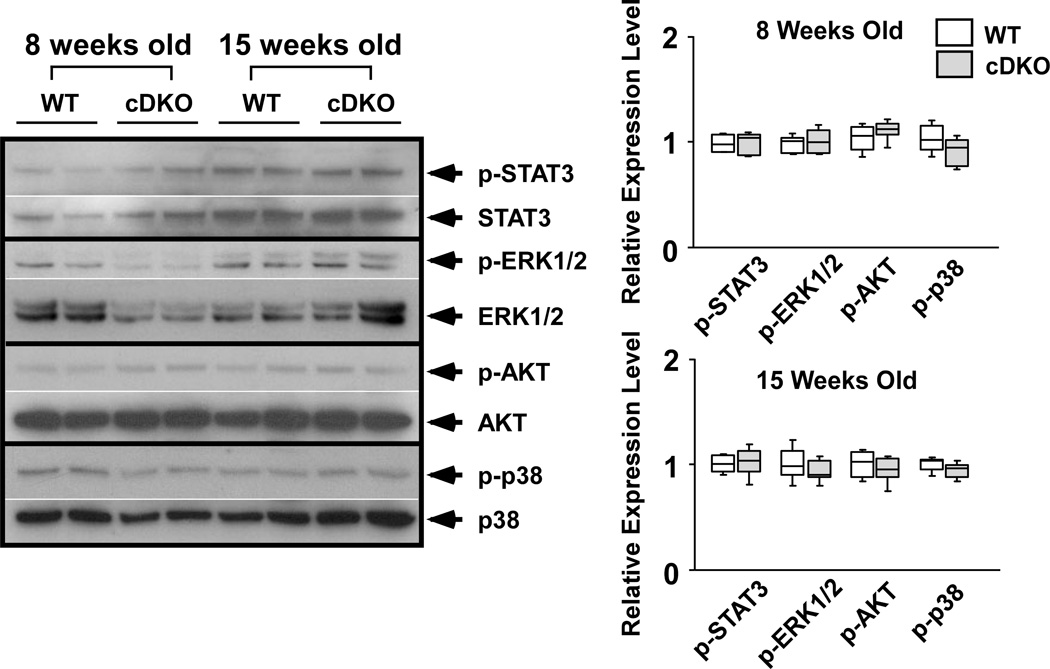
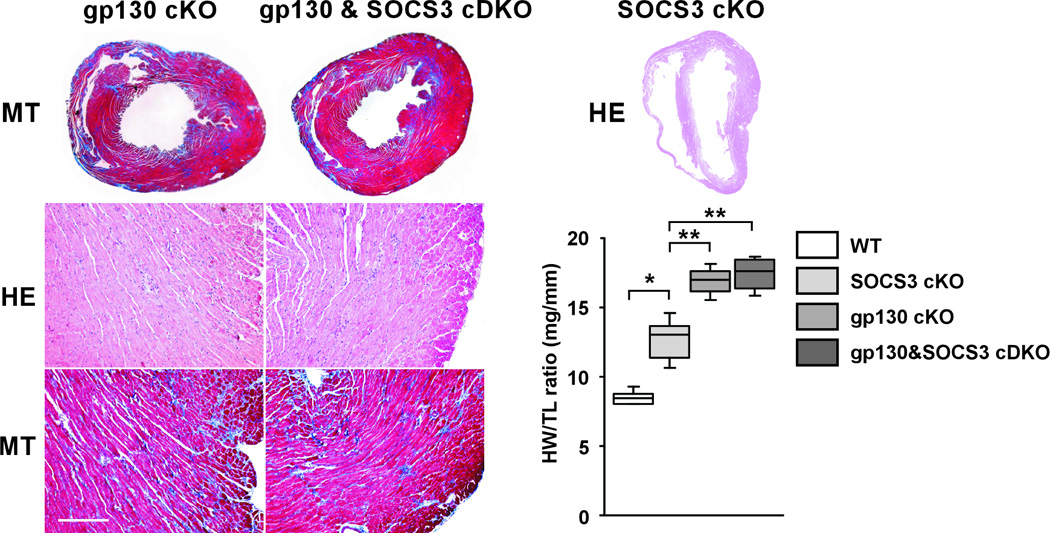
Methods and results: We generated cardiac-specific SOCS3 knockout (SOCS3 cKO) mice. These mice showed increased activation of gp130 downstream signaling targets (STAT3, ERK1/2, AKT, and p38) from 15 weeks of age and developed cardiac dysfunction from approximately 25 weeks of age with signs of heart failure. Surprisingly, SOCS3 cKO failing hearts had minimal histological abnormalities with intact myofibril ultrastructure. In addition, Ca(2+) transients were significantly increased in SOCS3 cKO failing hearts compared with wild-type hearts. We also found that Ser23/24 residues of troponin I were hypophosphorylated in SOCS3 cKO hearts before the manifestation of cardiac dysfunction. These data suggested the presence of abnormalities in myofilament Ca(2+) sensitivity in SOCS3 cKO mice. In addition to the contractile dysfunction, we found various ventricular arrhythmias in SOCS3 cKO nonfailing hearts accompanied by a sarcoplasmic reticulum Ca(2+) overload. To determine the contribution of gp130 signaling to the cardiac phenotype that occurs with SOCS3 deficiency, we generated cardiac-specific gp130 and SOCS3 double KO mice. Double KO mice lived significantly longer and had different histological abnormalities when compared with SOCS3 cKO mice, thus demonstrating the importance of gp130 signaling in the SOCS3 cKO cardiac phenotype.
Conclusions: Our results demonstrate an important role of SOCS3 regulation on cardiac gp130 signaling in the pathogenesis of contractile dysfunction and ventricular arrhythmias.
Figures



Similar articles
-
Innate defense mechanism against virus infection within the cardiac myocyte requiring gp130-STAT3 signaling.Circulation. 2006 Nov 28;114(22):2364-73. doi: 10.1161/CIRCULATIONAHA.106.642454. Epub 2006 Nov 13. Circulation. 2006. PMID: 17101849
-
Cardiac Ablation of SOCS3 Aggravates DOCA-Salt-Induced Hypertrophic Remodeling by Activation of Gp130-Dependent Signaling in Mice.Cell Physiol Biochem. 2018;47(1):140-150. doi: 10.1159/000489757. Epub 2018 May 10. Cell Physiol Biochem. 2018. PMID: 29763909
-
Suppressor of cytokine signaling-3 is a biomechanical stress-inducible gene that suppresses gp130-mediated cardiac myocyte hypertrophy and survival pathways.J Clin Invest. 2001 Nov;108(10):1459-67. doi: 10.1172/JCI13939. J Clin Invest. 2001. PMID: 11714737 Free PMC article.
-
Survival pathways in hypertrophy and heart failure: the gp130-STAT3 axis.Basic Res Cardiol. 2007 Jul;102(4):279-97. doi: 10.1007/s00395-007-0658-z. Epub 2007 May 29. Basic Res Cardiol. 2007. Corrected and republished in: Basic Res Cardiol. 2007 Sep;102(5):393-411. doi: 10.1007/s00395-007-0674-z PMID: 17530315 Corrected and republished. Review.
-
Survival pathways in hypertrophy and heart failure: the gp130-STAT axis.Basic Res Cardiol. 2007 Sep;102(5):393-411. doi: 10.1007/s00395-007-0674-z. Basic Res Cardiol. 2007. PMID: 17918316 Review.
Cited by
-
Inhibitory effects of suppressor of cytokine signaling 3 on inflammatory cytokine expression and migration and proliferation of IL-6/IFN-γ-induced vascular smooth muscle cells.J Huazhong Univ Sci Technolog Med Sci. 2013 Oct;33(5):615-622. doi: 10.1007/s11596-013-1168-x. Epub 2013 Oct 20. J Huazhong Univ Sci Technolog Med Sci. 2013. PMID: 24142708
-
Pathogenesis of SARS-CoV-2 induced cardiac injury from the perspective of the virus.J Mol Cell Cardiol. 2020 Oct;147:12-17. doi: 10.1016/j.yjmcc.2020.08.002. Epub 2020 Aug 6. J Mol Cell Cardiol. 2020. PMID: 32771409 Free PMC article. No abstract available.
-
STAT3 activity is necessary and sufficient for the development of immune-mediated myocarditis in mice and promotes progression to dilated cardiomyopathy.EMBO Mol Med. 2013 Apr;5(4):572-90. doi: 10.1002/emmm.201201876. Epub 2013 Mar 5. EMBO Mol Med. 2013. PMID: 23460527 Free PMC article.
-
Differential STAT3 signaling in the heart: Impact of concurrent signals and oxidative stress.JAKSTAT. 2012 Apr 1;1(2):101-10. doi: 10.4161/jkst.19776. JAKSTAT. 2012. PMID: 23904970 Free PMC article.
-
p42/p44-MAPK and PI3K are sufficient for IL-6 family cytokines/gp130 to signal to hypertrophy and survival in cardiomyocytes in the absence of JAK/STAT activation.Cell Signal. 2013 Apr;25(4):898-909. doi: 10.1016/j.cellsig.2012.12.008. Epub 2012 Dec 23. Cell Signal. 2013. PMID: 23268184 Free PMC article.
References
-
- Ernst M. Acquiring signalling specificity from the cytokine receptor gp130. Trends Genet. 2004;20:23–32. - PubMed
-
- Hilfiker-Kleiner D, Shukla P, Klein G, Schaefer A, Stapel B, Hoch M, Muller W, Scherr M, Theilmeier G, Ernst M, Hilfiker A, Drexler H. Continuous glycoprotein-130-mediated signal transducer and activator of transcription-3 activation promotes inflammation, left ventricular rupture, and adverse outcome in subacute myocardial infarction. Circulation. 2010;122:145–155. - PubMed
-
- Yajima T, Knowlton KU. Viral myocarditis: From the perspective of the virus. Circulation. 2009;119:2615–2624. - PubMed
-
- Hirota H, Chen J, Betz UA, Rajewsky K, Gu Y, Ross J, Jr, Muller W, Chien KR. Loss of a gp130 cardiac muscle cell survival pathway is a critical event in the onset of heart failure during biomechanical stress. Cell. 1999;97:189–198. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
