

Practice Guideline
doi: 10.1038/nrc3144.
Rethinking ovarian cancer: recommendations for improving outcomes
Affiliations
- PMID: 21941283
- PMCID: PMC3380637
- DOI: 10.1038/nrc3144
Item in Clipboard
Practice Guideline
Rethinking ovarian cancer: recommendations for improving outcomes
Nat Rev Cancer.
.
Abstract
There have been major advances in our understanding of the cellular and molecular biology of the human malignancies that are collectively referred to as ovarian cancer. At a recent Helene Harris Memorial Trust meeting, an international group of researchers considered actions that should be taken to improve the outcome for women with ovarian cancer. Nine major recommendations are outlined in this Opinion article.
Trial registration: ClinicalTrials.gov NCT00262847 NCT00434642 NCT00483782.
Figures
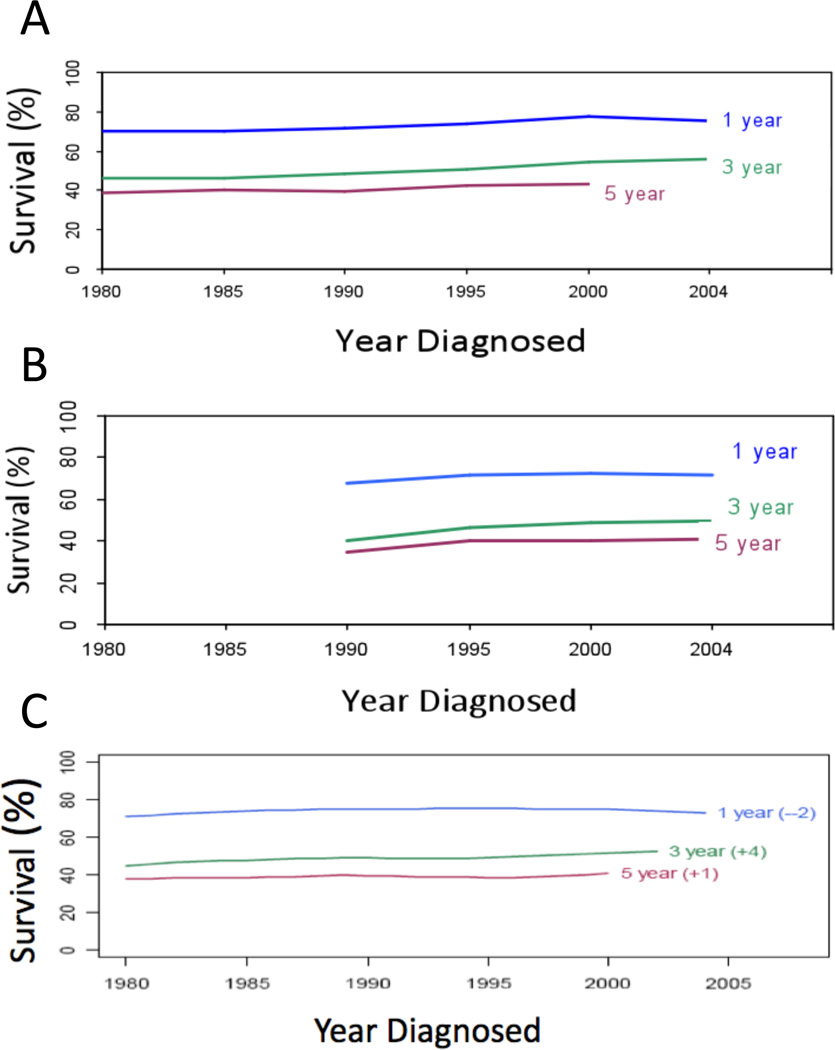
One-, three- and five-year survival post-diagnosis of ovarian cancer patients over the past 20 years. Data from: A) Surveillance, Epidemiology and End Results (SEER, 1980–2004); B) The Cancer Council of Victoria, Victoria, Australia (1990–2004); C) The Cheryl Brown Outcomes Unit, British Columbia, Canada (1980–2004).
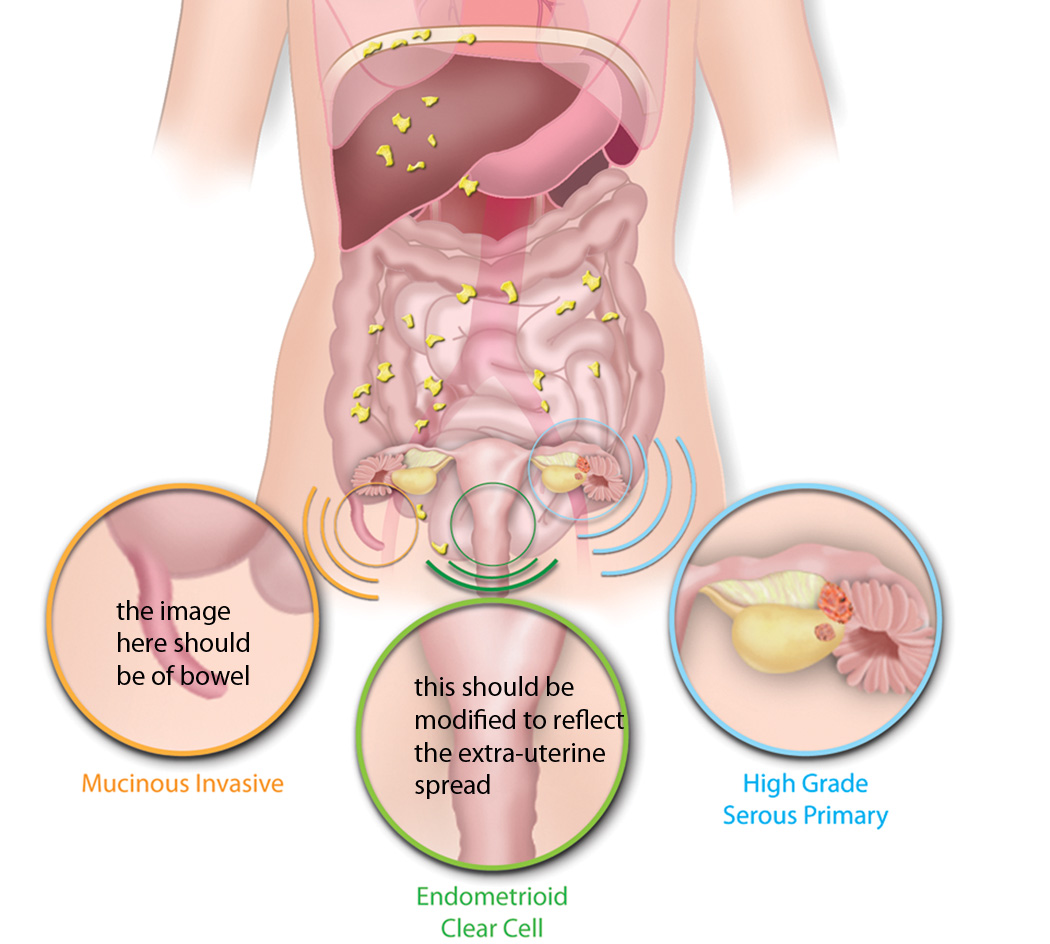
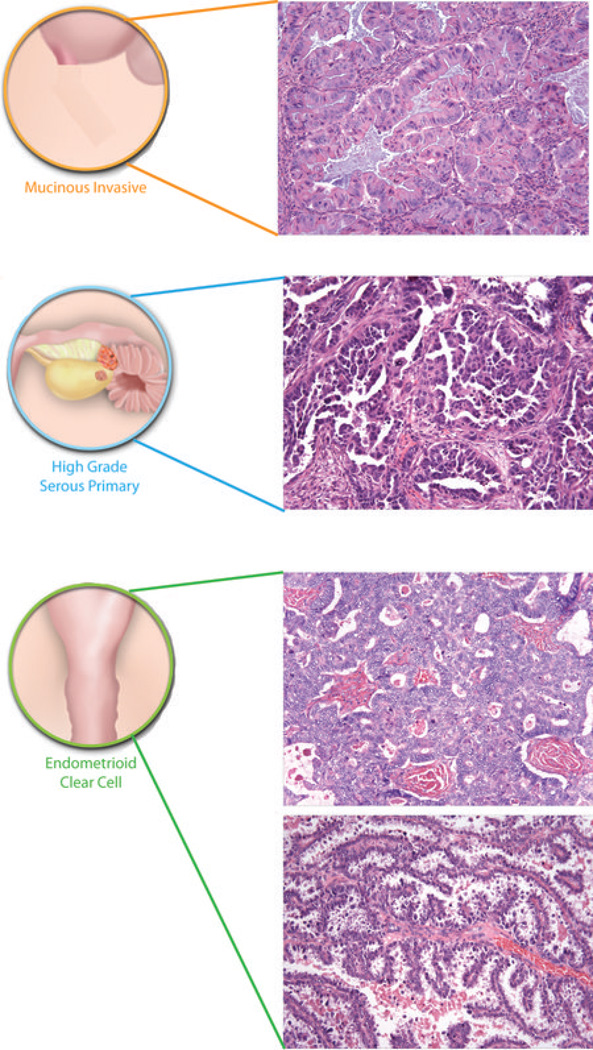
Ovarian cancer is a collective term for invasive cancers derived from different tissues. A majority of invasive mucinous ovarian cancers are metastases to the ovary, often from the gastrointestinal tract including colon (Co), appendix (Ap) or stomach (St). Endometrioid and clear cell ovarian cancers are derived from endometriosis, which in turn is associated with retrograde menstruation (blue arrow) from the endometrium (En). High grade serous ovarian cancers are derived from the surface of the ovary (Ov) and/or distal fallopian tube (FT) - the relative contribution that the two sites make to these tumours remains unclear. Benign and low malignant potential (borderline) tumours are not included in the diagram. Such tumours are thought to be of ovarian origin, however, the originating cells are not defined and their derivation may be revised in the future. Histological images courtesy of R. Drapkin, Dana-Farber Cancer Institute, USA, and C. Crum, Brigham and Women's Hospital, USA.
Ovarian cancer is a collective term for invasive cancers derived from different tissues. A majority of invasive mucinous ovarian cancers are metastases to the ovary, often from the gastrointestinal tract including colon (Co), appendix (Ap) or stomach (St). Endometrioid and clear cell ovarian cancers are derived from endometriosis, which in turn is associated with retrograde menstruation (blue arrow) from the endometrium (En). High grade serous ovarian cancers are derived from the surface of the ovary (Ov) and/or distal fallopian tube (FT) - the relative contribution that the two sites make to these tumours remains unclear. Benign and low malignant potential (borderline) tumours are not included in the diagram. Such tumours are thought to be of ovarian origin, however, the originating cells are not defined and their derivation may be revised in the future. Histological images courtesy of R. Drapkin, Dana-Farber Cancer Institute, USA, and C. Crum, Brigham and Women's Hospital, USA.
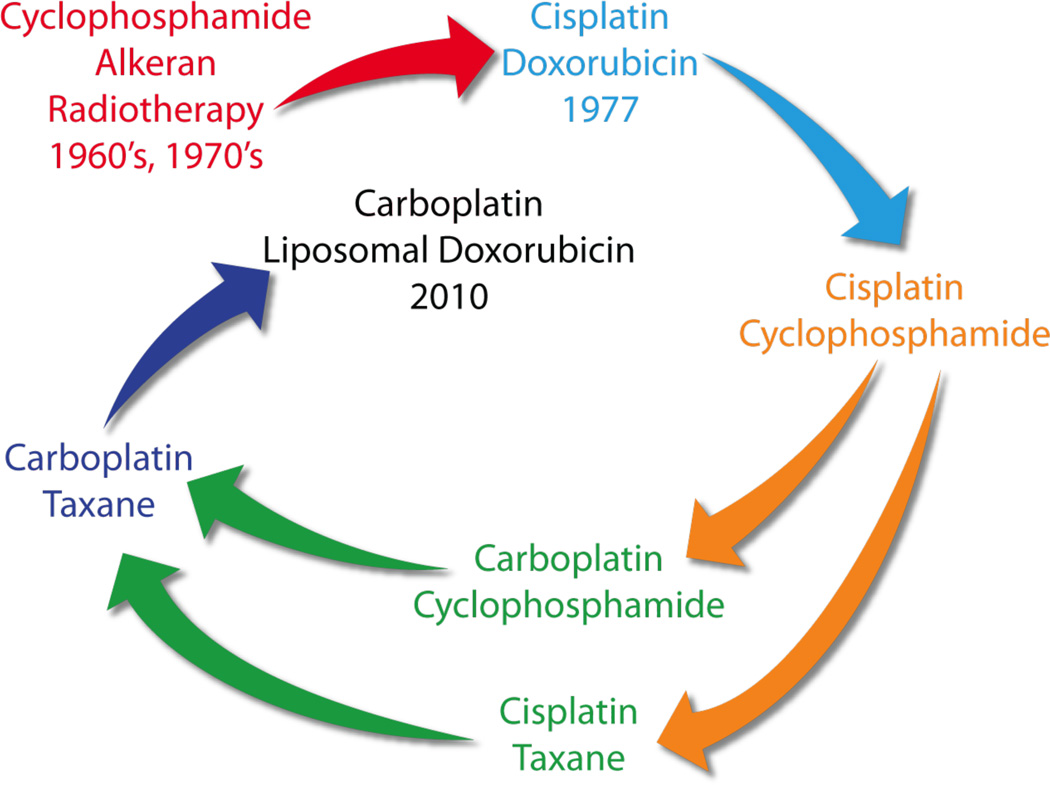
It has proved difficult to progress beyond platinum-based therapy, which was introduced in the late 1970s and remains standard of care. Cisplatin and subsequently carboplatin, which has a lower toxicity profile, have been combined with other agents, including taxanes. Most recently, liposomal doxorubicin has become commonly used with carboplatin, especially in a relapse setting. It is notable that the combination of carboplatin and liposomal doxorubicin involve similar drugs to those used in the mid-70s, albeit with reduced side-effects. It is likely that ovarian cancer treatment will evolve significantly in the coming years with the introduction of molecularly targeted agents, such as the poly(ADP-ribose) polymerase PARP inhibitors, histotype-specific treatments, and dose dense regimes, including use of weekly taxane.
Similar articles
-
Current research and treatment for epithelial ovarian cancer. A Position Paper from the Helene Harris Memorial Trust.Eur J Cancer. 2003 Sep;39(13):1818-27. doi: 10.1016/s0959-8049(03)00511-2. Eur J Cancer. 2003. PMID: 12932658
-
Targeted therapies for treatment of recurrent ovarian cancer.Clin Adv Hematol Oncol. 2014 Mar;12(3):158-62. Clin Adv Hematol Oncol. 2014. PMID: 24927263 Review.
-
Current treatment and clinical trials in ovarian cancer.Expert Opin Investig Drugs. 2010 Apr;19(4):521-34. doi: 10.1517/13543781003647966. Expert Opin Investig Drugs. 2010. PMID: 20367193 Review.
-
10th Biennial Helene Harris Memorial Trust meeting.Cancer Res. 2006 Mar 15;66(6):2904-6. doi: 10.1158/0008-5472.CAN-05-2093. Cancer Res. 2006. PMID: 16540635
-
Clinical trials referral resource. Clinical trials in ovarian cancer; Part 1.Oncology (Williston Park). 2002 Nov;16(11):1498-9, 1504, 1506-7. Oncology (Williston Park). 2002. PMID: 12469928 No abstract available.
Cited by
-
Enhancing delivery of small molecule and cell-based therapies for ovarian cancer using advanced delivery strategies.Adv Ther (Weinh). 2020 Nov;3(11):2000144. doi: 10.1002/adtp.202000144. Epub 2020 Aug 16. Adv Ther (Weinh). 2020. PMID: 33709016 Free PMC article.
-
Immune Tumor Microenvironment in Ovarian Cancer Ascites.Int J Mol Sci. 2022 Sep 14;23(18):10692. doi: 10.3390/ijms231810692. Int J Mol Sci. 2022. PMID: 36142615 Free PMC article. Review.
-
Ovarian cancer treatment: The end of empiricism?Cancer. 2015 Sep 15;121(18):3203-11. doi: 10.1002/cncr.29481. Epub 2015 Jun 10. Cancer. 2015. PMID: 26096019 Free PMC article. Review.
-
CDKN3 knockdown reduces cell proliferation, invasion and promotes apoptosis in human ovarian cancer.Int J Clin Exp Pathol. 2015 May 1;8(5):4535-44. eCollection 2015. Int J Clin Exp Pathol. 2015. PMID: 26191143 Free PMC article.
-
Up-regulation of CD44 in the development of metastasis, recurrence and drug resistance of ovarian cancer.Oncotarget. 2015 Apr 20;6(11):9313-26. doi: 10.18632/oncotarget.3220. Oncotarget. 2015. PMID: 25823654 Free PMC article.
References
-
- McGuire WP. Maintenance therapy for ovarian cancer: of Helsinki and Hippocrates. J Clin Oncol. 2009;27:4633–4634. - PubMed
-
- Omura G, et al. A randomized trial of cyclophosphamide and doxorubicin with or without cisplatin in advanced ovarian carcinoma. A Gynecologic Oncology Group Study. Cancer. 1986;57:1725–1730. - PubMed
-
- Piek JM, et al. Dysplastic changes in prophylactically removed Fallopian tubes of women predisposed to developing ovarian cancer. J Pathol. 2001;195:451–456. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- P50 CA83639/CA/NCI NIH HHS/United States
- P30 CA016672/CA/NCI NIH HHS/United States
- R01 CA085289/CA/NCI NIH HHS/United States
- P50 CA105009/CA/NCI NIH HHS/United States
- R01 CA111882/CA/NCI NIH HHS/United States
- RC2GM092599/GM/NIGMS NIH HHS/United States
- P50 CA098258/CA/NCI NIH HHS/United States
- U54 CA151668/CA/NCI NIH HHS/United States
- G0601891/MRC_/Medical Research Council/United Kingdom
- U01 CA151461/CA/NCI NIH HHS/United States
- 15601/CRUK_/Cancer Research UK/United Kingdom
- P50 CA083639/CA/NCI NIH HHS/United States
- U01 CA152990/CA/NCI NIH HHS/United States
- CA85289/CA/NCI NIH HHS/United States
- G0501974/MRC_/Medical Research Council/United Kingdom
- CA109298/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
