

Mechanisms of myocardial infarction in women without angiographically obstructive coronary artery disease
- PMID: 21900087
- PMCID: PMC3619391
- DOI: 10.1161/CIRCULATIONAHA.111.026542
Mechanisms of myocardial infarction in women without angiographically obstructive coronary artery disease
Abstract
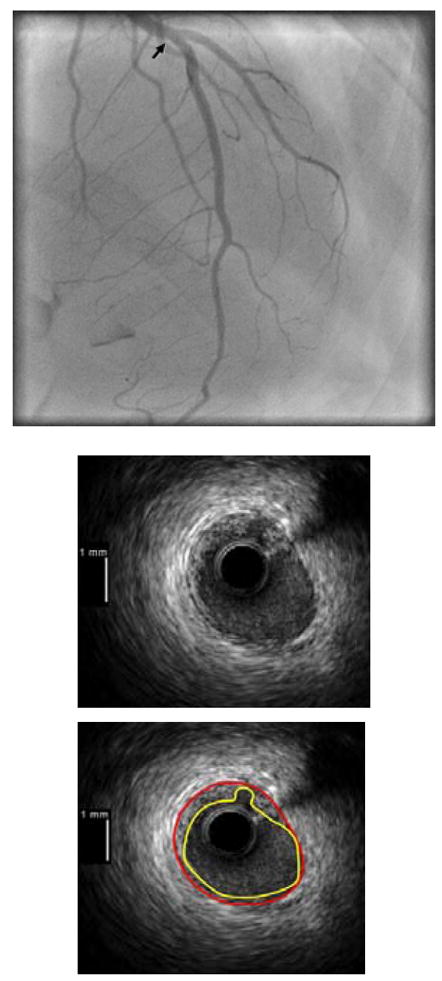
Background: There is no angiographically demonstrable obstructive coronary artery disease (CAD) in a significant minority of patients with myocardial infarction, particularly women. We sought to determine the mechanism(s) of myocardial infarction in this setting using multiple imaging techniques.
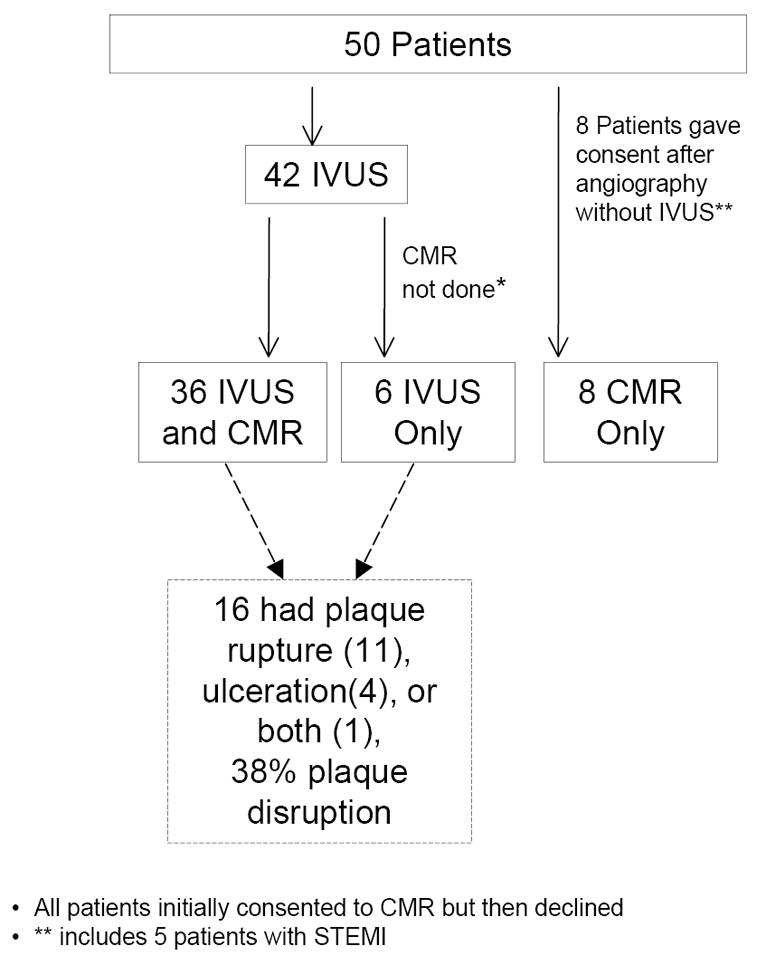
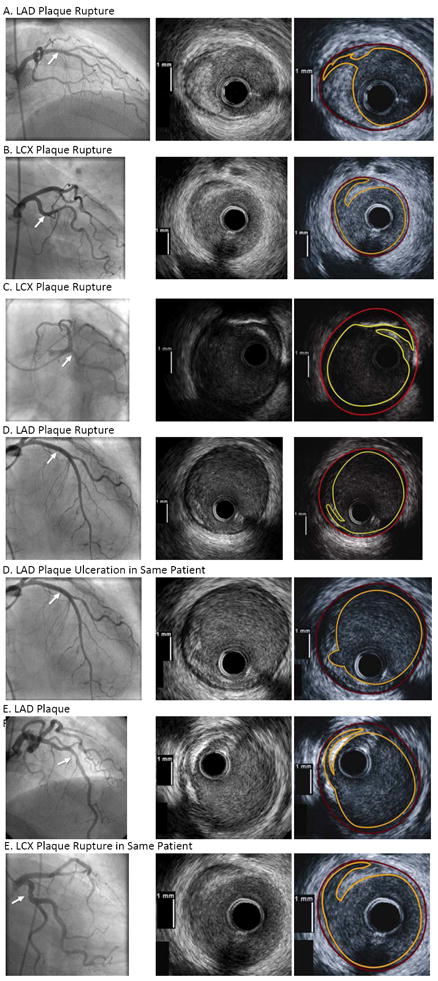
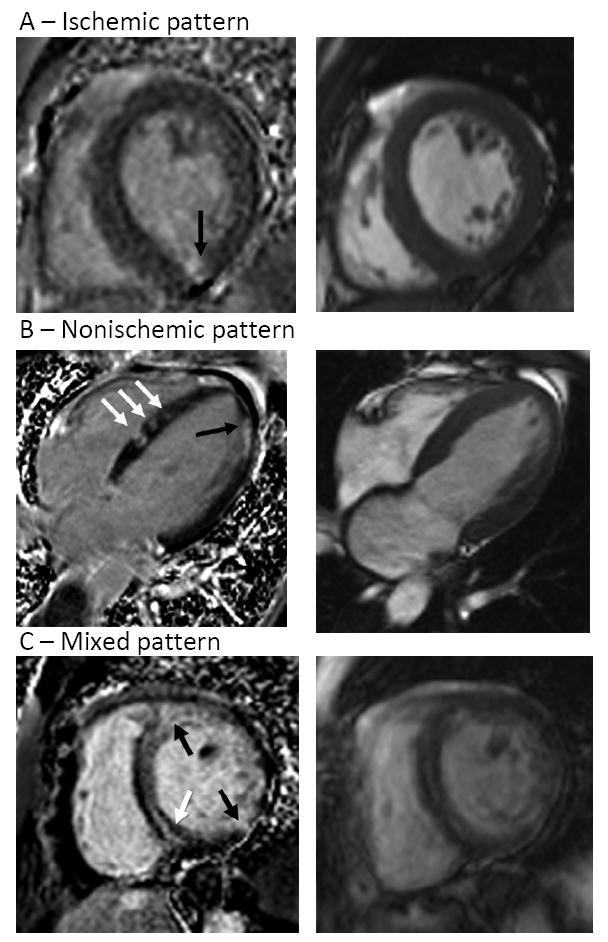
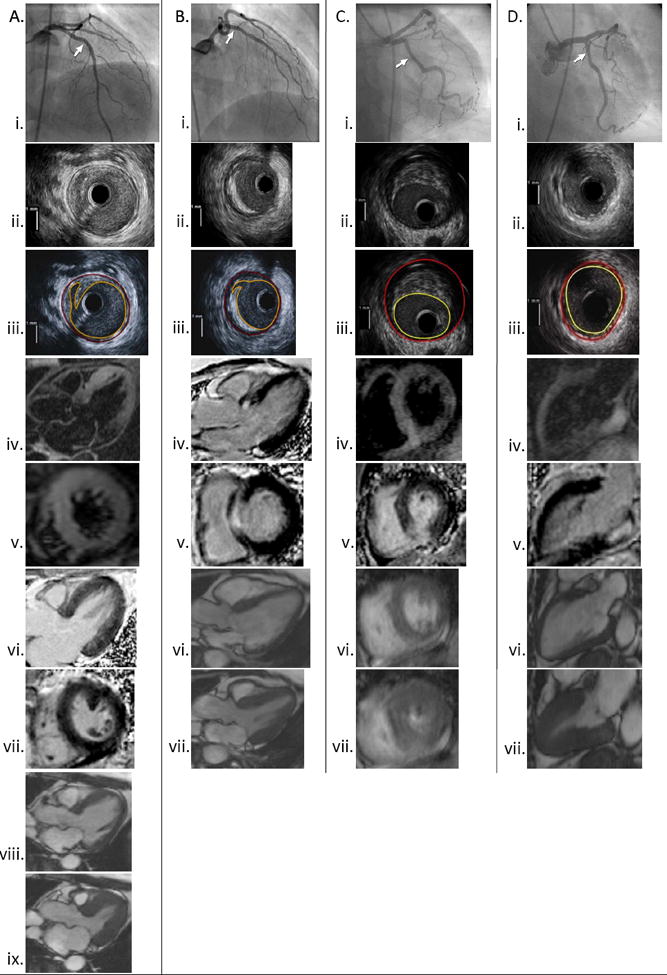
Methods and results: Women with myocardial infarction were enrolled prospectively, before angiography, if possible. Women with ≥50% angiographic stenosis or use of vasospastic agents were excluded. Intravascular ultrasound was performed during angiography; cardiac magnetic resonance imaging was performed within 1 week. Fifty women (age, 57±13 years) had median peak troponin of 1.60 ng/mL; 11 had ST-segment elevation. Median diameter stenosis of the worst lesion was 20% by angiography; 15 patients (30%) had normal angiograms. Plaque disruption was observed in 16 of 42 patients (38%) undergoing intravascular ultrasound. There were abnormal myocardial cardiac magnetic resonance imaging findings in 26 of 44 patients (59%) undergoing cardiac magnetic resonance imaging, late gadolinium enhancement (LGE) in 17 patients, and T2 signal hyperintensity indicating edema in 9 additional patients. The most common LGE pattern was ischemic (transmural/subendocardial). Nonischemic LGE patterns (midmyocardial/subepicardial) were also observed. Although LGE was infrequent with plaque disruption, T2 signal hyperintensity was common with plaque disruption.
Conclusions: Plaque rupture and ulceration are common in women with myocardial infarction without angiographically demonstrable obstructive coronary artery disease. In addition, LGE is common in this cohort of women, with an ischemic pattern of injury most evident. Vasospasm and embolism are possible mechanisms of ischemic LGE without plaque disruption. Intravascular ultrasound and cardiac magnetic resonance imaging provide complementary mechanistic insights into female myocardial infarction patients without obstructive coronary artery disease and may be useful in identifying potential causes and therapies. Clinical Trial Registration- URL: http://www.clinicaltrials.gov. Unique identifier: NCT00798122.
Conflict of interest statement
Figures
Comment in
-
What causes myocardial infarction in women without obstructive coronary artery disease?Circulation. 2011 Sep 27;124(13):1404-6. doi: 10.1161/CIRCULATIONAHA.111.055855. Circulation. 2011. PMID: 21947933 Free PMC article. No abstract available.
-
Letter by Chen and Zhang regarding article, "mechanisms of myocardial infarction in women without angiographically obstructive coronary artery disease".Circulation. 2012 Aug 7;126(6):e81; author reply e83. doi: 10.1161/CIRCULATIONAHA.111.076893. Circulation. 2012. PMID: 22869863 No abstract available.
-
Letter by Ward and Figtree article, "mechanisms of myocardial infarction in women without angiographically obstructive coronary artery disease".Circulation. 2012 Aug 7;126(6):e82; author reply e83. doi: 10.1161/CIRCULATIONAHA.111.077925. Circulation. 2012. PMID: 22869864 No abstract available.
Similar articles
-
Mechanisms of Myocardial Infarction in Patients With Nonobstructive Coronary Artery Disease: Results From the Optical Coherence Tomography Study.JACC Cardiovasc Imaging. 2019 Nov;12(11 Pt 1):2210-2221. doi: 10.1016/j.jcmg.2018.08.022. Epub 2018 Oct 17. JACC Cardiovasc Imaging. 2019. PMID: 30343070
-
Characteristics of plaque disruption by intravascular ultrasound in women presenting with myocardial infarction without obstructive coronary artery disease.Am Heart J. 2014 May;167(5):715-22. doi: 10.1016/j.ahj.2014.01.011. Epub 2014 Feb 26. Am Heart J. 2014. PMID: 24766982
-
Stress Cardiac MRI in Women With Myocardial Infarction and Nonobstructive Coronary Artery Disease.Clin Cardiol. 2016 Oct;39(10):596-602. doi: 10.1002/clc.22571. Epub 2016 Jul 26. Clin Cardiol. 2016. PMID: 27459149 Free PMC article.
-
Myocardial infarction without obstructive coronary artery disease.Curr Opin Cardiol. 2012 Nov;27(6):655-60. doi: 10.1097/HCO.0b013e3283583247. Curr Opin Cardiol. 2012. PMID: 22941122 Review.
-
Acute myocardial infarction with no obstructive coronary atherosclerosis: mechanisms and management.Eur Heart J. 2015 Feb 21;36(8):475-81. doi: 10.1093/eurheartj/ehu469. Epub 2014 Dec 18. Eur Heart J. 2015. PMID: 25526726 Review.
Cited by
-
Impact of Guideline-Directed Drug Therapy after ST-Elevation Myocardial Infarction on Outcome in Young Patients-Age and Sex-Specific Factors.J Clin Med. 2024 Jun 27;13(13):3788. doi: 10.3390/jcm13133788. J Clin Med. 2024. PMID: 38999354 Free PMC article.
-
Myocardial infarction or acute coronary syndrome with non-obstructive coronary arteries and sudden cardiac death: a missing connection.Europace. 2020 Sep 1;22(9):1303-1310. doi: 10.1093/europace/euaa156. Europace. 2020. PMID: 32894280 Free PMC article. Review.
-
Gender-related differences in men and women with ST-segment elevation myocardial infarction and incomplete infarct-related artery flow restoration: a multicenter national registry.Postepy Kardiol Interwencyjnej. 2018;14(4):356-362. doi: 10.5114/aic.2018.79865. Epub 2018 Dec 11. Postepy Kardiol Interwencyjnej. 2018. PMID: 30603025 Free PMC article.
-
Seasonal and circadian patterns of myocardial infarction by coronary artery disease status and sex in the ACTION Registry-GWTG.Int J Cardiol. 2019 Jan 1;274:16-20. doi: 10.1016/j.ijcard.2018.08.103. Epub 2018 Sep 1. Int J Cardiol. 2019. PMID: 30217419 Free PMC article.
-
Diagnostic Puzzles and Cause-Targeted Treatment Strategies in Myocardial Infarction with Non-Obstructive Coronary Arteries: An Updated Review.J Clin Med. 2023 Sep 26;12(19):6198. doi: 10.3390/jcm12196198. J Clin Med. 2023. PMID: 37834842 Free PMC article. Review.
References
-
- Hochman JS, Tamis JE, Thompson TD, Weaver WD, White HD, VandeWerf F, Aylward P, Topol EJ, Califf RM. Sex, clinical presentation, and outcome in patients with acute coronary syndromes. N Engl J Med. 1999;341:226–232. - PubMed
-
- Gehrie ER, Reynolds HR, Chen AY, Neelon BH, Roe MT, Gibler WB, Ohman EM, Newby LK, Peterson ED, Hochman JS. Characterization and outcomes of women and men with non-ST-segment elevation myocardial infarction and nonobstructive coronary artery disease: results of the CRUSADE quality improvement initiative. Am Heart J. 2009;158:688–694. - PubMed
-
- Chokshi NP, Iqbal SN, Berger RL, Hochman JS, Feit F, Slater JN, Pena-Sing I, Yatskar L, Keller NM, Babaev A, Attubato MJ, Reynolds HR. Sex and race are associated with the absence of epicardial coronary artery obstructive disease at angiography in patients with acute coronary syndromes. Clin Cardiol. 2010;33:495–501. - PMC - PubMed
-
- Nageh T, Sherwood RA, Wainwright RJ, Shah AM, Thomas MR. The clinical relevance of raised cardiac troponin I in the absence of significant angiographic coronary artery disease. Int J Cardiol. 2005;100:325–330. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
