

The incidence, root-causes, and outcomes of adverse events in surgical units: implication for potential prevention strategies
- PMID: 21599915
- PMCID: PMC3127749
- DOI: 10.1186/1754-9493-5-13
The incidence, root-causes, and outcomes of adverse events in surgical units: implication for potential prevention strategies
Abstract
Background: We need to know the scale and underlying causes of surgical adverse events (AEs) in order to improve the safety of care in surgical units. However, there is little recent data. Previous record review studies that reported on surgical AEs in detail are now more than ten years old. Since then surgical technology and quality assurance have changed rapidly. The objective of this study was to provide more recent data on the incidence, consequences, preventability, causes and potential strategies to prevent AEs among hospitalized patients in surgical units.
Methods: A structured record review study of 7,926 patient records was carried out by trained nurses and medical specialist reviewers in 21 Dutch hospitals. The aim was to determine the presence of AEs during hospitalizations in 2004 and to consider how far they could be prevented. Of all AEs, the consequences, responsible medical specialty, causes and potential prevention strategies were identified. Surgical AEs were defined as AEs attributable to surgical treatment and care processes and were selected for analysis in detail.
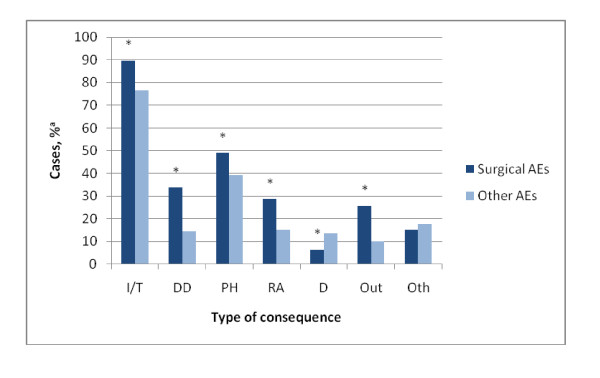
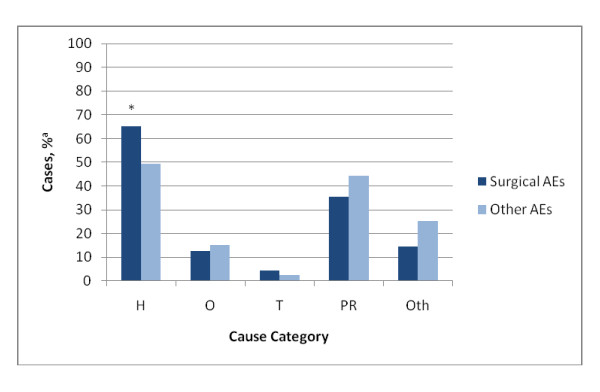
Results: Surgical AEs occurred in 3.6% of hospital admissions and represented 65% of all AEs. Forty-one percent of the surgical AEs was considered to be preventable. The consequences of surgical AEs were more severe than for other types of AEs, resulting in more permanent disability, extra treatment, prolonged hospital stay, unplanned readmissions and extra outpatient visits. Almost 40% of the surgical AEs were infections, 23% bleeding, and 22% injury by mechanical, physical or chemical cause. Human factors were involved in the causation of 65% of surgical AEs and were considered to be preventable through quality assurance and training.
Conclusions: Surgical AEs occur more often than other types of AEs, are more often preventable and their consequences are more severe. Therefore, surgical AEs have a major impact on the burden of AEs during hospitalizations. These findings concur with the results from previous studies. However, evidence-based solutions to reduce surgical AEs are increasingly available. Interventions directed at human causes are recommended to improve the safety of surgical care. Examples are team training and the surgical safety checklist. In addition, specific strategies are needed to improve appropriate use of antibiotic prophylaxis and sustainable implementation of hygiene guidelines to reduce infections.
Figures
Similar articles
-
Examining Causes and Prevention Strategies of Adverse Events in Deceased Hospital Patients: A Retrospective Patient Record Review Study in the Netherlands.J Patient Saf. 2021 Jun 1;17(4):282-289. doi: 10.1097/PTS.0000000000000586. J Patient Saf. 2021. PMID: 30896559
-
Exploring unplanned ICU admissions: a systematic review.JBI Libr Syst Rev. 2011;9(25):925-959. doi: 10.11124/01938924-201109250-00001. JBI Libr Syst Rev. 2011. PMID: 27820505
-
Incidence of adverse events, preventability and mortality in gynaecological hospital admissions: A systematic review and meta-analysis.Aust N Z J Obstet Gynaecol. 2019 Apr;59(2):195-200. doi: 10.1111/ajo.12937. Epub 2019 Jan 20. Aust N Z J Obstet Gynaecol. 2019. PMID: 30663036
-
Incidence and preventability of adverse events requiring intensive care admission: a systematic review.J Eval Clin Pract. 2012 Apr;18(2):485-97. doi: 10.1111/j.1365-2753.2010.01612.x. Epub 2011 Jan 6. J Eval Clin Pract. 2012. PMID: 21210898 Review.
-
The epidemiology of medical errors: a review of the literature.Wien Klin Wochenschr. 2003 May 30;115(10):318-25. doi: 10.1007/BF03041483. Wien Klin Wochenschr. 2003. PMID: 12800445 Review.
Cited by
-
Assessment of Anaesthesia Teams' Non-Technical Skills in Clinical Practice before and after Simulation-Based Team Training: A Quasiexperimental Study.Anesthesiol Res Pract. 2024 Jul 5;2024:2021671. doi: 10.1155/2024/2021671. eCollection 2024. Anesthesiol Res Pract. 2024. PMID: 39006532 Free PMC article.
-
The anatomy of safe surgical teams: an interview-based qualitative study among members of surgical teams at tertiary referral hospitals in Norway.Patient Saf Surg. 2024 Feb 19;18(1):7. doi: 10.1186/s13037-024-00389-w. Patient Saf Surg. 2024. PMID: 38374077 Free PMC article.
-
Hemopatch® is effective and safe to use: real-world data from a prospective European registry study.Updates Surg. 2022 Oct;74(5):1521-1531. doi: 10.1007/s13304-022-01353-y. Epub 2022 Aug 20. Updates Surg. 2022. PMID: 35986865 Free PMC article.
-
La définition des moments critiques et non critiques en salle d'opération : une étude de consensus Delphi modifiée.Can J Anaesth. 2020 Aug;67(8):949-958. doi: 10.1007/s12630-020-01688-3. Epub 2020 May 6. Can J Anaesth. 2020. PMID: 32377936 English.
-
Enhanced Recovery After Surgery Guidelines and Hospital Length of Stay, Readmission, Complications, and Mortality: A Meta-Analysis of Randomized Clinical Trials.JAMA Netw Open. 2024 Jun 3;7(6):e2417310. doi: 10.1001/jamanetworkopen.2024.17310. JAMA Netw Open. 2024. PMID: 38888922 Free PMC article.
References
-
- Baker GR, Norton PG, Flintoft V, Blais R, Brown A, Cox J, Etchells E, Ghali WA, Hébert P, Majumdar SR, O'Beirne M, Palacios-Derflingher L, Reid RJ, Sheps S, Tamblyn R. The Canadian Adverse Events Study: the incidence of adverse events among hospital patients in Canada. CMAJ. 2004;170:1678–86. doi: 10.1503/cmaj.1040498. - DOI - PMC - PubMed
-
- Davis P, Lay-Yee R, Briant R, Ali W, Scott A, Schug S. Adverse events in New Zealand public hospitals I: occurrence and impact. N Z Med J. 2002;115:U271. - PubMed
-
- Davis P, Lay-Yee R, Briant R, Ali W, Scott A, Schug S. Adverse events in New Zealand public hospitals II: preventability and clinical context. N Z Med J. 2003;116:U624. - PubMed
LinkOut - more resources
Full Text Sources
