

Biochemical markers of ongoing joint damage in rheumatoid arthritis--current and future applications, limitations and opportunities
- PMID: 21539724
- PMCID: PMC3132026
- DOI: 10.1186/ar3280
Biochemical markers of ongoing joint damage in rheumatoid arthritis--current and future applications, limitations and opportunities
Abstract
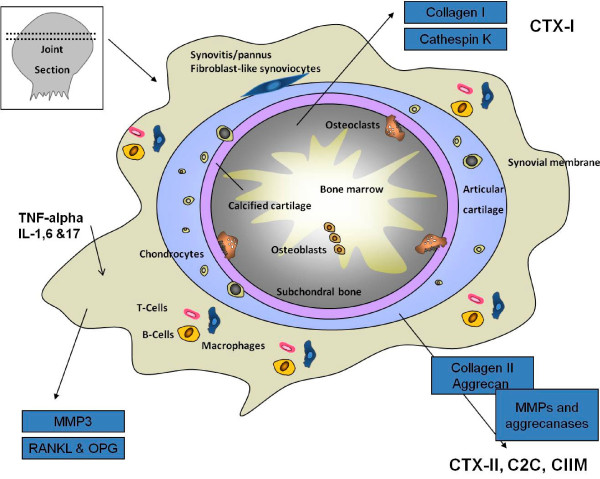
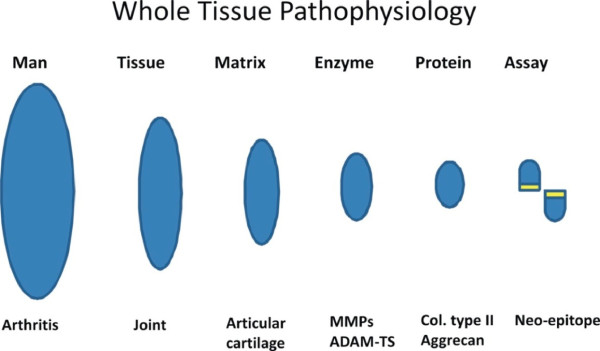
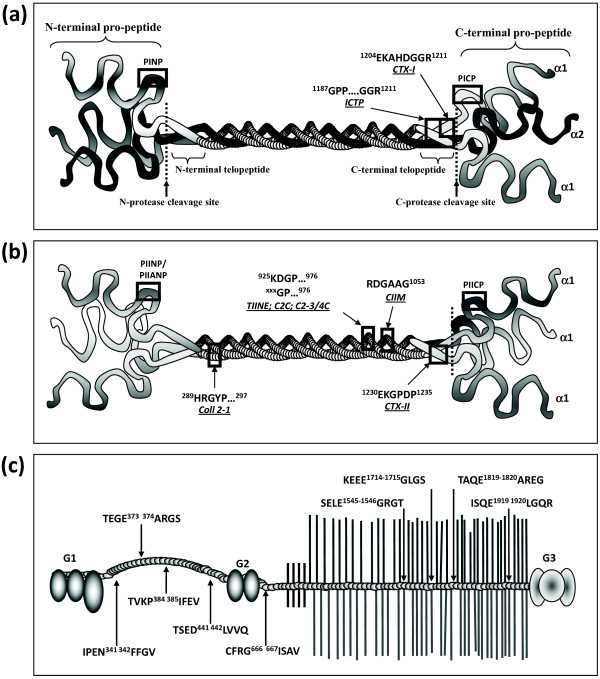
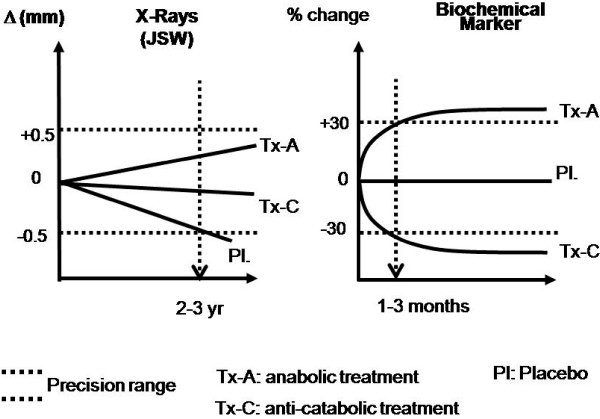
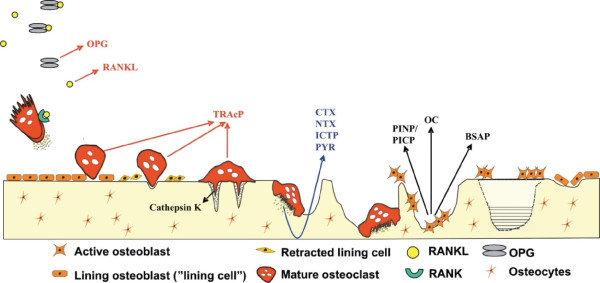
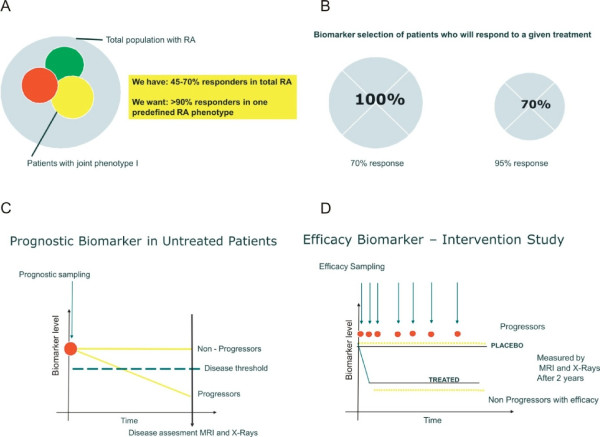
Rheumatoid arthritis (RA) is a chronic systemic autoimmune disease associated with potentially debilitating joint inflammation, as well as altered skeletal bone metabolism and co-morbid conditions. Early diagnosis and aggressive treatment to control disease activity offers the highest likelihood of preserving function and preventing disability. Joint inflammation is characterized by synovitis, osteitis, and/or peri-articular osteopenia, often accompanied by development of subchondral bone erosions, as well as progressive joint space narrowing. Biochemical markers of joint cartilage and bone degradation may enable timely detection and assessment of ongoing joint damage, and their use in facilitating treatment strategies is under investigation. Early detection of joint damage may be assisted by the characterization of biochemical markers that identify patients whose joint damage is progressing rapidly and who are thus most in need of aggressive treatment, and that, alone or in combination, identify those individuals who are likely to respond best to a potential treatment, both in terms of limiting joint damage and relieving symptoms. The aims of this review are to describe currently available biochemical markers of joint metabolism in relation to the pathobiology of joint damage and systemic bone loss in RA; to assess the limitations of, and need for additional, novel biochemical markers in RA and other rheumatic diseases, and the strategies used for assay development; and to examine the feasibility of advancement of personalized health care using biochemical markers to select therapeutic agents to which a patient is most likely to respond.
Figures
Similar articles
-
Osteitis and synovitis, but not bone erosion, is associated with proteoglycan loss and microstructure damage in the cartilage of patients with rheumatoid arthritis.Ann Rheum Dis. 2014 Jun;73(6):1101-6. doi: 10.1136/annrheumdis-2012-202850. Epub 2013 Apr 26. Ann Rheum Dis. 2014. PMID: 23625980
-
The clinical features of rheumatoid arthritis.Eur J Radiol. 1998 May;27 Suppl 1:S18-24. doi: 10.1016/s0720-048x(98)00038-2. Eur J Radiol. 1998. PMID: 9652497 Review.
-
The interplay between inflammation and metabolism in rheumatoid arthritis.Cell Death Dis. 2015 Sep 17;6(9):e1887. doi: 10.1038/cddis.2015.246. Cell Death Dis. 2015. PMID: 26379192 Free PMC article. Review.
-
Biochemical markers of joint tissue turnover in early rheumatoid arthritis.Clin Exp Rheumatol. 2003 Sep-Oct;21(5 Suppl 31):S54-8. Clin Exp Rheumatol. 2003. PMID: 14969051 Review.
-
Noninvasive techniques for assessing skeletal changes in inflammatory arthritis: bone biomarkers.Curr Opin Rheumatol. 2004 Jul;16(4):428-34. doi: 10.1097/01.moo.0000127830.72761.00. Curr Opin Rheumatol. 2004. PMID: 15201607 Review.
Cited by
-
Can quaternary ammonium methacrylates inhibit matrix MMPs and cathepsins?Dent Mater. 2015 Feb;31(2):e25-32. doi: 10.1016/j.dental.2014.10.006. Epub 2014 Nov 22. Dent Mater. 2015. PMID: 25467953 Free PMC article.
-
Expression of synovial fluid biomarkers in patients with knee osteoarthritis and meniscus injury.Exp Ther Med. 2017 Aug;14(2):1609-1613. doi: 10.3892/etm.2017.4636. Epub 2017 Jun 21. Exp Ther Med. 2017. PMID: 28810626 Free PMC article.
-
Low-Grade Inflammatory Mediators and Metalloproteinases Yield Synchronous and Delayed Responses to Mechanical Joint Loading.Cartilage. 2024 Dec;15(4):417-427. doi: 10.1177/19476035231193089. Epub 2023 Aug 24. Cartilage. 2024. PMID: 37614184 Free PMC article.
-
Serum adenosine deaminase in patients with rheumatoid arthritis treated with methotrexate.J Res Pharm Pract. 2012 Oct;1(2):72-6. doi: 10.4103/2279-042X.108374. J Res Pharm Pract. 2012. PMID: 24991593 Free PMC article.
-
Osteopontin, osteoprotegerin and musculoskeletal ultrasound findings in first-degree relatives of rheumatoid arthritis: potential markers of preclinical disease.BMC Musculoskelet Disord. 2024 Mar 5;25(1):195. doi: 10.1186/s12891-024-07291-7. BMC Musculoskelet Disord. 2024. PMID: 38443806 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
