

Therapeutic surgical management of palpable melanoma groin metastases: superficial or combined superficial and deep groin lymph node dissection
- PMID: 21537867
- PMCID: PMC3192282
- DOI: 10.1245/s10434-011-1741-0
Therapeutic surgical management of palpable melanoma groin metastases: superficial or combined superficial and deep groin lymph node dissection
Abstract
Background: Management of patients with clinically detectable lymph node metastasis to the groin is by ilioinguinal or combined superficial and deep groin dissection (CGD) according to most literature, but in practice superficial groin dissection (SGD) only is still performed in some centers. The aim of this study is to evaluate the experience in CGD versus SGD patients in our center.
Methods: Between 1991 and 2009, 121 therapeutic CGD and 48 SGD were performed in 169 melanoma patients with palpable groin metastases at our institute. Median follow-up was 20 and, for survivors, 45 months.
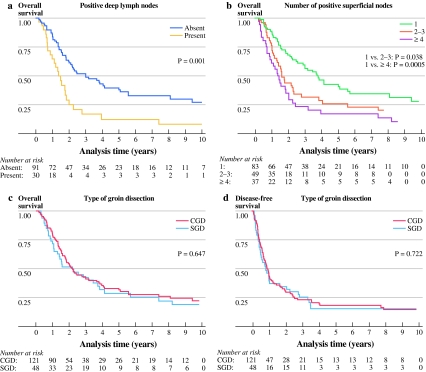
Results: In this heterogeneous group of patients, overall (OS) and disease-free survival, local control rates, and morbidity rates were not significantly different between CGD and SGD patients. However, CGD patients had a trend towards more chronic lymphedema. Superficial lymph node ratio, the number of positive superficial lymph nodes, and the presence of deep nodes were prognostic factors for survival. CGD patients with involved deep lymph nodes (24.8%) had estimated 5-year OS of 12% compared with 40% with no involved deep lymph nodes (p=0.001). Preoperative computed tomography (CT) scan had high negative predictive value of 91% for detection of pelvic nodal involvement.
Conclusions: This study demonstrated that survival and local control do not differ for patients with palpable groin metastases treated by CGD or SGD. Patients without pathological iliac nodes on CT might safely undergo SGD, while CGD might be reserved for patients with multiple positive nodes on SGD and/or positive deep nodes on CT scan.
Figures
Similar articles
-
Risk Factors for Positive Deep Pelvic Nodal Involvement in Patients with Palpable Groin Melanoma Metastases: Can the Extent of Surgery be Safely Minimized? : A Retrospective, Multicenter Cohort Study.Ann Surg Oncol. 2015 Dec;22 Suppl 3:S1172-80. doi: 10.1245/s10434-015-4602-4. Epub 2015 May 27. Ann Surg Oncol. 2015. PMID: 26014150 Free PMC article.
-
Regional control and morbidity after superficial groin dissection in melanoma.Ann Surg Oncol. 2011 May;18(5):1453-9. doi: 10.1245/s10434-010-1450-0. Epub 2010 Dec 7. Ann Surg Oncol. 2011. PMID: 21136182 Free PMC article.
-
Deep lymph node metastases in the groin significantly affects prognosis, particularly in sentinel node-positive melanoma patients.Ann Surg Oncol. 2015 Jan;22(1):279-86. doi: 10.1245/s10434-014-3854-8. Epub 2014 Jul 10. Ann Surg Oncol. 2015. PMID: 25008028
-
Combined inguinal and pelvic lymph node dissection for stage III melanoma.Br J Surg. 1999 Dec;86(12):1493-8. doi: 10.1046/j.1365-2168.1999.01316.x. Br J Surg. 1999. PMID: 10594495 Review.
-
Results of radical dissection of the groin in patients with stage II melanoma and histologically proved metastases of the iliac or obturator lymph nodes, or both.Surg Gynecol Obstet. 1988 Jul;167(1):28-32. Surg Gynecol Obstet. 1988. PMID: 3289133 Review.
Cited by
-
Role of a skin bridge incision and prophylactic incisional negative-pressure wound therapy in the prevention of surgical site infection after inguinal lymph node dissection.Can J Surg. 2022 Oct 20;65(5):E688-E694. doi: 10.1503/cjs.005621. Print 2022 Sep-Oct. Can J Surg. 2022. PMID: 36265898 Free PMC article.
-
Preoperative ultrasound is not useful for identifying nodal metastasis in melanoma patients undergoing sentinel node biopsy: preoperative ultrasound in clinically node-negative melanoma.Ann Surg Oncol. 2012 Apr;19(4):1100-6. doi: 10.1245/s10434-011-2172-7. Epub 2011 Dec 23. Ann Surg Oncol. 2012. PMID: 22193886 Free PMC article.
-
Laparoscopically assisted ilio-inguinal lymph node dissection versus inguinal lymph node dissection in melanoma.Melanoma Manag. 2020 Jul 21;7(2):MMT42. doi: 10.2217/mmt-2019-0023. Melanoma Manag. 2020. PMID: 32821374 Free PMC article.
-
Malignant melanoma: evolving practice management in an era of increasingly effective systemic therapies.Curr Probl Surg. 2022 Jan;59(1):101030. doi: 10.1016/j.cpsurg.2021.101030. Epub 2021 Jul 7. Curr Probl Surg. 2022. PMID: 35033317 Free PMC article. Review. No abstract available.
-
Neoadjuvant Systemic Therapy (NAST) in Patients with Melanoma: Surgical Considerations by the International Neoadjuvant Melanoma Consortium (INMC).Ann Surg Oncol. 2022 Jun;29(6):3694-3708. doi: 10.1245/s10434-021-11236-y. Epub 2022 Jan 28. Ann Surg Oncol. 2022. PMID: 35089452
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
