

Intensive care unit-acquired weakness (ICUAW) and muscle wasting in critically ill patients with severe sepsis and septic shock
- PMID: 21475702
- PMCID: PMC3060654
- DOI: 10.1007/s13539-010-0010-6
Intensive care unit-acquired weakness (ICUAW) and muscle wasting in critically ill patients with severe sepsis and septic shock
Abstract
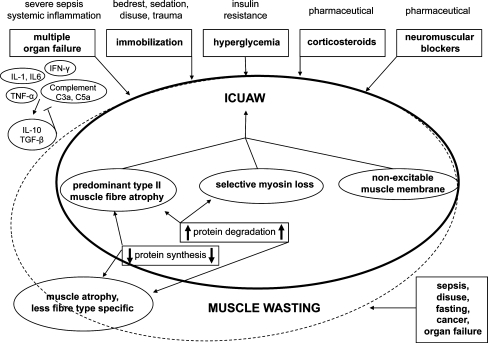
Sepsis presents a major health care problem and remains one of the leading causes of death within the intensive care unit (ICU). Therapeutic approaches against severe sepsis and septic shock focus on early identification. Adequate source control, administration of antibiotics, preload optimization by fluid resuscitation and further hemodynamic stabilisation using vasopressors whenever appropriate are considered pivotal within the early-golden-hours of sepsis. However, organ dysfunction develops frequently in and represents a significant comorbidity of sepsis. A considerable amount of patients with sepsis will show signs of severe muscle wasting and/or ICU-acquired weakness (ICUAW), which describes a frequently observed complication in critically ill patients and refers to clinically weak ICU patients in whom there is no plausible aetiology other than critical illness. Some authors consider ICUAW as neuromuscular organ failure, caused by dysfunction of the motor unit, which consists of peripheral nerve, neuromuscular junction and skeletal muscle fibre. Electrophysiologic and/or biopsy studies facilitate further subclassification of ICUAW as critical illness myopathy, critical illness polyneuropathy or critical illness myoneuropathy, their combination. ICUAW may protract weaning from mechanical ventilation and impede rehabilitation measures, resulting in increased morbidity and mortality. This review provides an insight on the available literature on sepsis-mediated muscle wasting, ICUAW and their potential pathomechanisms.
Figures
Similar articles
-
Clinical review: intensive care unit acquired weakness.Crit Care. 2015 Aug 5;19(1):274. doi: 10.1186/s13054-015-0993-7. Crit Care. 2015. PMID: 26242743 Free PMC article. Review.
-
Hyperlactacidemia as a risk factor for intensive care unit-acquired weakness in critically ill adult patients.Muscle Nerve. 2021 Jul;64(1):77-82. doi: 10.1002/mus.27248. Epub 2021 Apr 21. Muscle Nerve. 2021. PMID: 33831220
-
An official American Thoracic Society Clinical Practice guideline: the diagnosis of intensive care unit-acquired weakness in adults.Am J Respir Crit Care Med. 2014 Dec 15;190(12):1437-46. doi: 10.1164/rccm.201411-2011ST. Am J Respir Crit Care Med. 2014. PMID: 25496103
-
Propofol as a Risk Factor for ICU-Acquired Weakness in Septic Patients with Acute Respiratory Failure.Can J Neurol Sci. 2017 May;44(3):295-303. doi: 10.1017/cjn.2016.424. Epub 2017 Jan 16. Can J Neurol Sci. 2017. PMID: 28091345
-
Intensive care unit-acquired weakness and the COVID-19 pandemic: A clinical review.PM R. 2022 Feb;14(2):227-238. doi: 10.1002/pmrj.12757. Epub 2022 Jan 31. PM R. 2022. PMID: 35014183 Review.
Cited by
-
Reliability of ultrasound measurements of quadriceps muscle thickness in critically ill patients.BMC Anesthesiol. 2018 Dec 27;18(1):205. doi: 10.1186/s12871-018-0647-9. BMC Anesthesiol. 2018. PMID: 30591032 Free PMC article.
-
Explorative Clustering of the Nitrogen Balance Trajectory in Critically Ill Patients: A Preliminary post hoc Analysis of a Single-Center Prospective Observational Study.Ann Nutr Metab. 2023;79(5):460-468. doi: 10.1159/000532126. Epub 2023 Oct 9. Ann Nutr Metab. 2023. PMID: 37812913 Free PMC article.
-
Effect of Early Rehabilitation in the Intensive Care Unit by a Dedicated Therapist Using a Rehabilitation Protocol: A Single-center Retrospective Study.Prog Rehabil Med. 2021 Aug 4;6:20210030. doi: 10.2490/prm.20210030. eCollection 2021. Prog Rehabil Med. 2021. PMID: 34395932 Free PMC article.
-
Functional Status in ICU Survivors and Out of Hospital Outcomes: A Cohort Study.Crit Care Med. 2016 May;44(5):869-79. doi: 10.1097/CCM.0000000000001627. Crit Care Med. 2016. PMID: 26929191 Free PMC article.
-
The ChIP-seq-defined networks of Bcl-3 gene binding support its required role in skeletal muscle atrophy.PLoS One. 2012;7(12):e51478. doi: 10.1371/journal.pone.0051478. Epub 2012 Dec 10. PLoS One. 2012. PMID: 23251550 Free PMC article.
References
-
- American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med 1992;20:864–74. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
