

Acute kidney injury: what's the prognosis?
- PMID: 21343898
- PMCID: PMC3547642
- DOI: 10.1038/nrneph.2011.13
Acute kidney injury: what's the prognosis?
Abstract
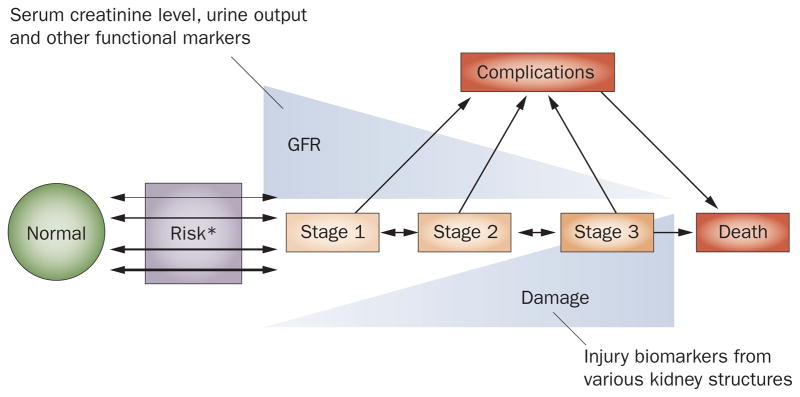
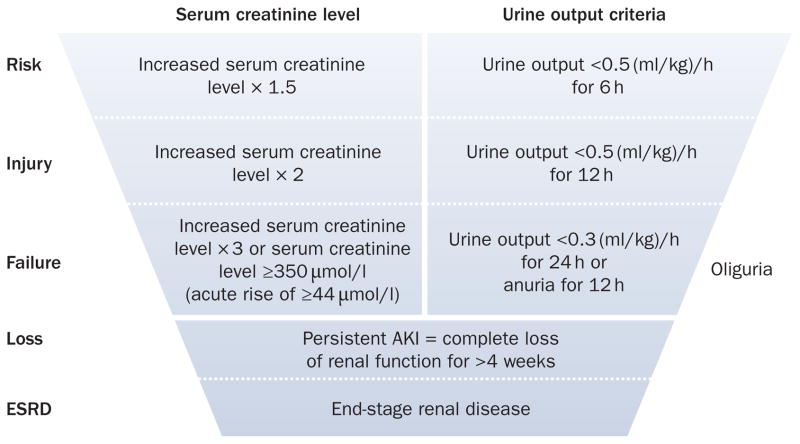
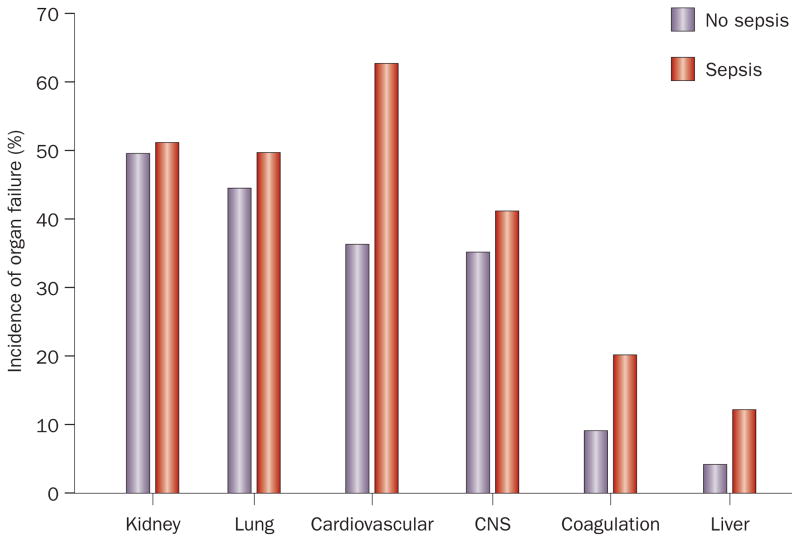
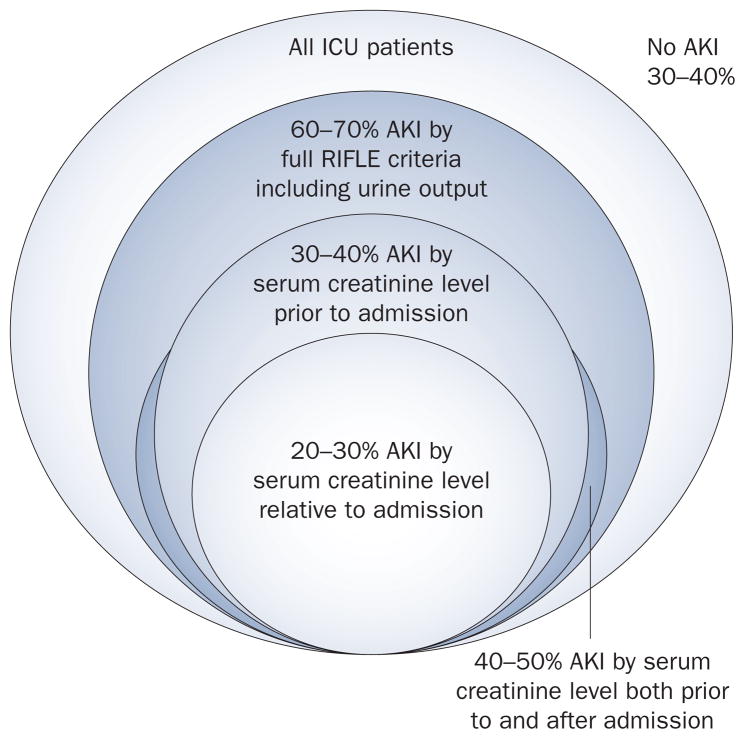
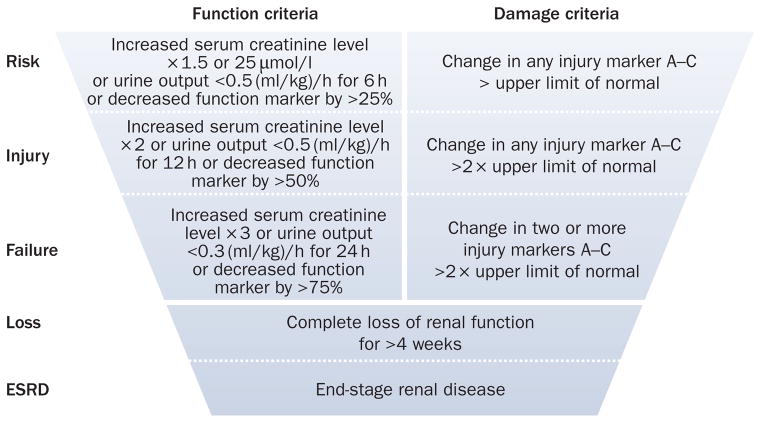
Acute kidney injury (AKI) is common (especially during critical illness), increasing in incidence, and is associated with considerable morbidity and mortality. The Risk, Injury, Failure, Loss, and End-stage renal disease (RIFLE) classification currently provides a standardized estimate of incidence and outcomes from AKI. Despite advances in the understanding of the pathogenesis of human AKI, our ability to assess kidney function is limited and functional impairment poorly correlates with structural injury to the kidneys. Emerging novel biomarkers are, however, likely to further enhance risk stratification, facilitate early diagnosis, enable early enrollment in therapeutic trials, and assess prognosis. Sepsis remains the leading cause of AKI among the critically ill and over the past few years insights into the pathogenesis of AKI in sepsis are beginning to shift attention from renal blood flow to inflammation-mediated organ injury. Emerging evidence suggests that survivors of AKI incur long-term risks for developing chronic kidney disease and end-stage renal disease compared with those without AKI. Despite decades of research, no specific therapy for AKI other than supportive care currently exists and further work is required to better understand the pathogenesis of AKI during critical illness and to develop novel treatments.
Conflict of interest statement
R. Murugan and J. A. Kellum declare an association with the following company: Baxter. J. A. Kellum declares associations with the following companies: Alere, Abbott Laboratories, Astute Medical, Gambro. See the article online for full details of the relationships.
Figures
Similar articles
-
Our paper 20 years later: from acute renal failure to acute kidney injury--the metamorphosis of a syndrome.Intensive Care Med. 2015 Nov;41(11):1941-9. doi: 10.1007/s00134-015-3989-5. Epub 2015 Aug 22. Intensive Care Med. 2015. PMID: 26297119
-
Incidence, risk factors and outcome of acute kidney injury in critically ill children - a developing country perspective.Paediatr Int Child Health. 2017 Feb;37(1):35-41. doi: 10.1080/20469047.2015.1120409. Epub 2016 Jan 9. Paediatr Int Child Health. 2017. PMID: 26752169
-
Urinary biomarkers may provide prognostic information for subclinical acute kidney injury after cardiac surgery.J Thorac Cardiovasc Surg. 2018 Jun;155(6):2441-2452.e13. doi: 10.1016/j.jtcvs.2017.12.056. Epub 2017 Dec 22. J Thorac Cardiovasc Surg. 2018. PMID: 29366580
-
Acute kidney injury in critically ill newborns: what do we know? What do we need to learn?Pediatr Nephrol. 2009 Feb;24(2):265-74. doi: 10.1007/s00467-008-1060-2. Epub 2008 Dec 10. Pediatr Nephrol. 2009. PMID: 19082634 Free PMC article. Review.
-
Proteomic biomarkers for the early detection of acute kidney injury.Prilozi. 2012;33(1):27-48. Prilozi. 2012. PMID: 22952093 Review.
Cited by
-
Impact of feline AIM on the susceptibility of cats to renal disease.Sci Rep. 2016 Oct 12;6:35251. doi: 10.1038/srep35251. Sci Rep. 2016. PMID: 27731392 Free PMC article.
-
Impact on Outcomes across KDIGO-2012 AKI Criteria According to Baseline Renal Function.J Clin Med. 2019 Aug 28;8(9):1323. doi: 10.3390/jcm8091323. J Clin Med. 2019. PMID: 31466281 Free PMC article.
-
Association of Current Active Illnesses and Severe Acute Kidney Injury after COVID-19 Vaccines: A Real-World Study.Vaccines (Basel). 2022 Apr 29;10(5):706. doi: 10.3390/vaccines10050706. Vaccines (Basel). 2022. PMID: 35632462 Free PMC article.
-
ATG7 promotes autophagy in sepsis‑induced acute kidney injury and is inhibited by miR‑526b.Mol Med Rep. 2020 May;21(5):2193-2201. doi: 10.3892/mmr.2020.11001. Epub 2020 Feb 26. Mol Med Rep. 2020. PMID: 32323768 Free PMC article.
-
Searching for mechanisms that matter in early septic acute kidney injury: an experimental study.Crit Care. 2011;15(5):R256. doi: 10.1186/cc10517. Epub 2011 Oct 26. Crit Care. 2011. PMID: 22030145 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
