

Association between C reactive protein and coronary heart disease: mendelian randomisation analysis based on individual participant data
- PMID: 21325005
- PMCID: PMC3039696
- DOI: 10.1136/bmj.d548
Association between C reactive protein and coronary heart disease: mendelian randomisation analysis based on individual participant data
Abstract
Objective: To use genetic variants as unconfounded proxies of C reactive protein concentration to study its causal role in coronary heart disease.
Design: Mendelian randomisation meta-analysis of individual participant data from 47 epidemiological studies in 15 countries.
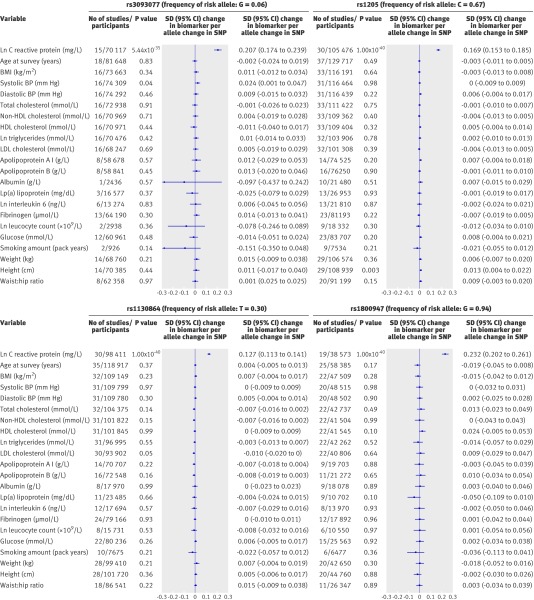
Participants: 194 418 participants, including 46 557 patients with prevalent or incident coronary heart disease. Information was available on four CRP gene tagging single nucleotide polymorphisms (rs3093077, rs1205, rs1130864, rs1800947), concentration of C reactive protein, and levels of other risk factors.
Main outcome measures: Risk ratios for coronary heart disease associated with genetically raised C reactive protein versus risk ratios with equivalent differences in C reactive protein concentration itself, adjusted for conventional risk factors and variability in risk factor levels within individuals.
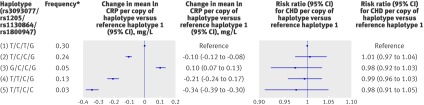
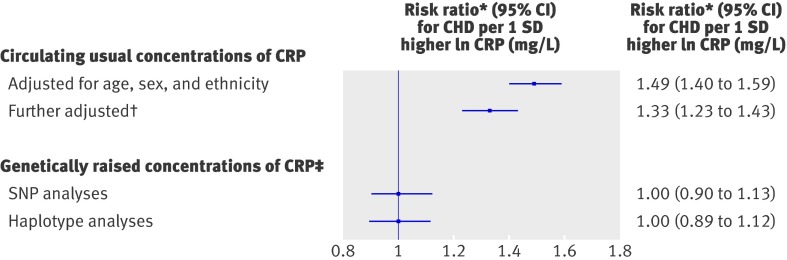
Results: CRP variants were each associated with up to 30% per allele difference in concentration of C reactive protein (P<10(-34)) and were unrelated to other risk factors. Risk ratios for coronary heart disease per additional copy of an allele associated with raised C reactive protein were 0.93 (95% confidence interval 0.87 to 1.00) for rs3093077; 1.00 (0.98 to 1.02) for rs1205; 0.98 (0.96 to 1.00) for rs1130864; and 0.99 (0.94 to 1.03) for rs1800947. In a combined analysis, the risk ratio for coronary heart disease was 1.00 (0.90 to 1.13) per 1 SD higher genetically raised natural log (ln) concentration of C reactive protein. The genetic findings were discordant with the risk ratio observed for coronary heart disease of 1.33 (1.23 to 1.43) per 1 SD higher circulating ln concentration of C reactive protein in prospective studies (P=0.001 for difference).
Conclusion: Human genetic data indicate that C reactive protein concentration itself is unlikely to be even a modest causal factor in coronary heart disease.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures

Comment in
-
C reactive protein and the risk of cardiovascular disease.BMJ. 2011 Feb 15;342:d144. doi: 10.1136/bmj.d144. BMJ. 2011. PMID: 21325003 No abstract available.
Similar articles
-
Association of CRP genetic variants with blood concentrations of C-reactive protein and colorectal cancer risk.Int J Cancer. 2015 Mar 1;136(5):1181-92. doi: 10.1002/ijc.29086. Epub 2014 Jul 28. Int J Cancer. 2015. PMID: 25043606 Free PMC article. Clinical Trial.
-
Genetic Loci associated with C-reactive protein levels and risk of coronary heart disease.JAMA. 2009 Jul 1;302(1):37-48. doi: 10.1001/jama.2009.954. JAMA. 2009. PMID: 19567438 Free PMC article.
-
Association of plasma C-reactive protein with ischaemic stroke: a Mendelian randomization study.Eur J Neurol. 2020 Mar;27(3):565-571. doi: 10.1111/ene.14113. Epub 2019 Nov 26. Eur J Neurol. 2020. PMID: 31692152
-
Evaluating the causal relevance of diverse risk markers: horizontal systematic review.BMJ. 2009 Nov 5;339:b4265. doi: 10.1136/bmj.b4265. BMJ. 2009. PMID: 19892791 Free PMC article. Review.
-
C-reactive protein and coronary heart disease: all said--is not it?Mediators Inflamm. 2014;2014:757123. doi: 10.1155/2014/757123. Epub 2014 Apr 7. Mediators Inflamm. 2014. PMID: 24808639 Free PMC article. Review.
Cited by
-
How does childhood maltreatment influence cardiovascular disease? A sequential causal mediation analysis.Int J Epidemiol. 2022 May 9;51(2):555-566. doi: 10.1093/ije/dyab085. Int J Epidemiol. 2022. PMID: 34041541 Free PMC article.
-
Diabetes, diabetic complications, and fracture risk.Curr Osteoporos Rep. 2015 Apr;13(2):106-15. doi: 10.1007/s11914-015-0260-5. Curr Osteoporos Rep. 2015. PMID: 25648962 Free PMC article. Review.
-
Visualization of atherosclerosis as detected by coronary artery calcium and carotid intima-media thickness reveals significant atherosclerosis in a cross-sectional study of psoriasis patients in a tertiary care center.J Transl Med. 2016 Jul 22;14(1):217. doi: 10.1186/s12967-016-0947-0. J Transl Med. 2016. PMID: 27448600 Free PMC article.
-
Sensitivity Analyses for Robust Causal Inference from Mendelian Randomization Analyses with Multiple Genetic Variants.Epidemiology. 2017 Jan;28(1):30-42. doi: 10.1097/EDE.0000000000000559. Epidemiology. 2017. PMID: 27749700 Free PMC article.
-
Association of inflammatory gene polymorphisms with mechanical heart valve reoperation.Springerplus. 2016 Jun 30;5(1):937. doi: 10.1186/s40064-016-2566-x. eCollection 2016. Springerplus. 2016. PMID: 27386381 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
- MC_U137686857/MRC_/Medical Research Council/United Kingdom
- G0100222/MRC_/Medical Research Council/United Kingdom
- RG/08/013/25942/BHF_/British Heart Foundation/United Kingdom
- G0801056/MRC_/Medical Research Council/United Kingdom
- UL1 RR025741/RR/NCRR NIH HHS/United States
- G0801566/MRC_/Medical Research Council/United Kingdom
- G0601966/MRC_/Medical Research Council/United Kingdom
- G7900510/MRC_/Medical Research Council/United Kingdom
- PG/07/083/22975/BHF_/British Heart Foundation/United Kingdom
- RG/07/008/23674/BHF_/British Heart Foundation/United Kingdom
- G19/35/MRC_/Medical Research Council/United Kingdom
- G8802774/MRC_/Medical Research Council/United Kingdom
- RG/08/008/25291/BHF_/British Heart Foundation/United Kingdom
- MC_U105260792/MRC_/Medical Research Council/United Kingdom
- G0700931/MRC_/Medical Research Council/United Kingdom
- G0902037/MRC_/Medical Research Council/United Kingdom
- 082178/WT_/Wellcome Trust/United Kingdom
- G0600705/MRC_/Medical Research Council/United Kingdom
- G0401527/MRC_/Medical Research Council/United Kingdom
- SP/08/007/23628/BHF_/British Heart Foundation/United Kingdom
- G1000143/MRC_/Medical Research Council/United Kingdom
- SP/08/007/BHF_/British Heart Foundation/United Kingdom
- FS05/125/BHF_/British Heart Foundation/United Kingdom
- RG/08/014/24067/BHF_/British Heart Foundation/United Kingdom
- MC_QA137933/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous