

Circulating stem cell vary with NYHA stage in heart failure patients
- PMID: 21029373
- PMCID: PMC4373363
- DOI: 10.1111/j.1582-4934.2010.01195.x
Circulating stem cell vary with NYHA stage in heart failure patients
Abstract
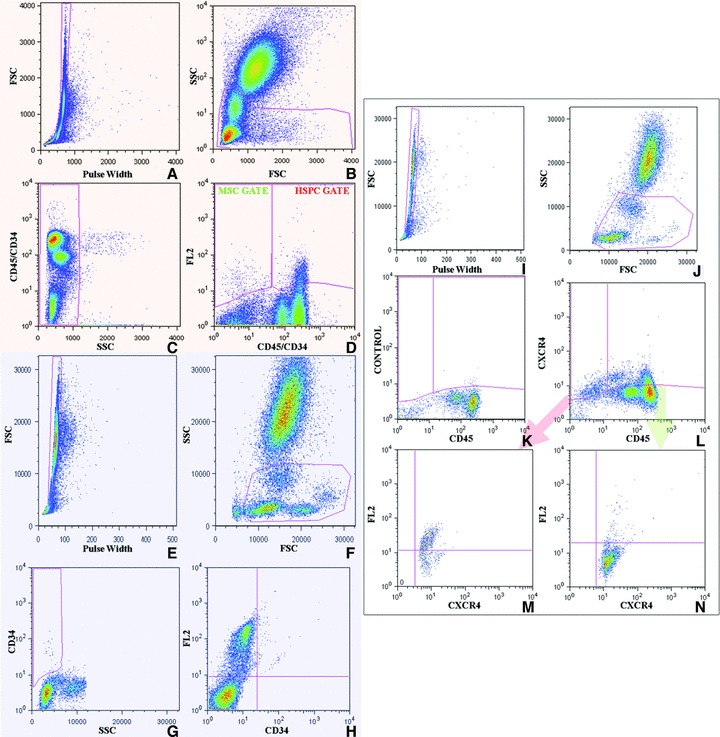
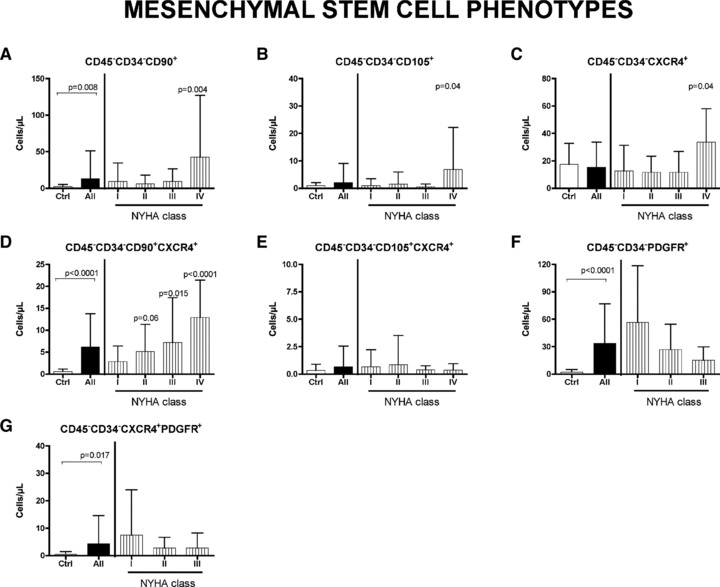
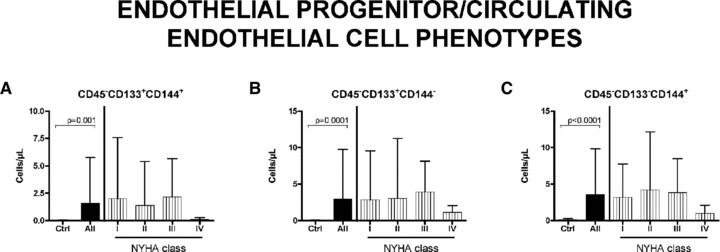
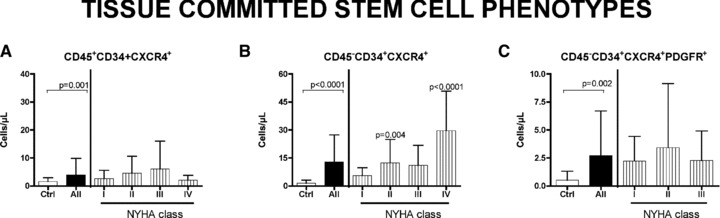
We have investigated the blood levels of sub-classes of stem cells (SCs) [mesenchymal stem cells (MSCs), haematopoietic stem cells (HSCs), endothelial progenitor cells/circulating endothelial cells (EPCs/CECs) and tissue-committed stem cells (TCSCs)] in heart failure (HF) patients at different stage of pathology and correlated it with plasmatic levels of proangiogenic cytokines. Peripheral blood level of SCs were analysed in 97 HF patients (24 in NYHA class I, 41 in class II, 17 in class III and 15 in class IV) and in 23 healthy controls. Plasmatic levels of PDGF-BB, bFGF, HGF, vascular endothelial growth factor (VEGF), SDF-1α, TNF-α and NTproBNP were also measured. Compared with healthy individuals, MSC, and in particular the sub-classes CD45(-) CD34(-) CD90(+) , CD45(-) CD34(-) CD105(+) and CD45(-) CD34(-) CXCR4(+) were significantly enhanced in NYHA class IV patients (16.8-, 6.4- and 2.7-fold, respectively). Level of CD45(-) CD34(-) CD90(+) CXCR4(+) cells progressively increased from class II to class IV (fold increases compared with controls: 8.5, 12 and 21.5, respectively). A significant involvement of CXCR4(+) subpopulation of HSC (CD45(+) CD34(+) CD90(+) CXCR4(+) , 1.4 versus 13.3 cells/μl in controls and NYHA class III patients, respectively) and TCSC (CD45(-) CD34(+) CXCR4(+) , 1.5 cells/ μl in controls versus 12.4 and 28.6 cells/μl in NYHA classes II and IV, respectively) were also observed. All tested cytokines were enhanced in HF patients. In particular, for PDGF-BB and SDF-1α we studied specific ligand/receptors pairs. Interestingly, the first one positively correlated with TCSCs expressing PDGFR (r = 0.52, P = 0.001), whereas the second one correlated with TCSCs (r = 0.34, P = 0.005) and with MSCs CD90(+) expressing CXCR4 (r = 0.39, P = 0.001). HF is characterized by the increase in the circulating levels of different MSC, HSC, EPC and TCSC subsets. Both the entity and kinetic of this process varied in distinct cell subsets. Specifically, differently from HSCs and EPCs/CECs, MSCs and TCSCs significantly increased with the progression of the disease, suggesting a possible distinct role of these cells in the pathophysiology of HF.
© 2011 The Authors Journal compilation © 2011 Foundation for Cellular and Molecular Medicine/Blackwell Publishing Ltd.
Figures


Similar articles
-
CD34+ and endothelial progenitor cells in patients with various degrees of congestive heart failure.Circulation. 2004 Sep 7;110(10):1209-12. doi: 10.1161/01.CIR.0000136813.89036.21. Epub 2004 Jul 12. Circulation. 2004. PMID: 15249502
-
Differential effect of ischaemic preconditioning on mobilisation and recruitment of haematopoietic and mesenchymal stem cells in porcine myocardial ischaemia-reperfusion.Thromb Haemost. 2010 Aug;104(2):376-84. doi: 10.1160/TH09-08-0558. Epub 2010 Mar 29. Thromb Haemost. 2010. PMID: 20352158
-
Value and level of circulating endothelial progenitor cells, angiogenesis factors and mononuclear cell apoptosis in patients with chronic kidney disease.Clin Exp Nephrol. 2013 Feb;17(1):83-91. doi: 10.1007/s10157-012-0664-9. Epub 2012 Jul 20. Clin Exp Nephrol. 2013. PMID: 22814956
-
Reviewing and updating the major molecular markers for stem cells.Stem Cells Dev. 2013 May 1;22(9):1455-76. doi: 10.1089/scd.2012.0637. Epub 2013 Jan 22. Stem Cells Dev. 2013. PMID: 23336433 Free PMC article. Review.
-
The Use of Hematopoietic Stem Cells for Heart Failure: A Systematic Review.Int J Mol Sci. 2024 Jun 17;25(12):6634. doi: 10.3390/ijms25126634. Int J Mol Sci. 2024. PMID: 38928341 Free PMC article. Review.
Cited by
-
Attenuation of hind-limb ischemia in mice with endothelial-like cells derived from different sources of human stem cells.PLoS One. 2013;8(3):e57876. doi: 10.1371/journal.pone.0057876. Epub 2013 Mar 5. PLoS One. 2013. PMID: 23472116 Free PMC article.
-
Modified Taohong Siwu decoction improves cardiac function after myocardial ischaemia and reperfusion in rats by promoting endogenous stem cell mobilization and regulating metabolites.Pharm Biol. 2022 Dec;60(1):1721-1731. doi: 10.1080/13880209.2022.2116054. Pharm Biol. 2022. PMID: 36086864 Free PMC article.
-
Anti-Inflammatory Fibronectin-AgNP for Regulation of Biological Performance and Endothelial Differentiation Ability of Mesenchymal Stem Cells.Int J Mol Sci. 2021 Aug 26;22(17):9262. doi: 10.3390/ijms22179262. Int J Mol Sci. 2021. PMID: 34502171 Free PMC article.
-
Distinct mobilization of circulating CD271+ mesenchymal progenitors from hematopoietic progenitors during aging and after myocardial infarction.Stem Cells Transl Med. 2012 Jun;1(6):462-8. doi: 10.5966/sctm.2011-0051. Epub 2012 Jun 5. Stem Cells Transl Med. 2012. PMID: 23197850 Free PMC article.
-
Molecular advances in reporter genes: the need to witness the function of stem cells in failing heart in vivo.Stem Cell Rev Rep. 2012 Jun;8(2):503-12. doi: 10.1007/s12015-011-9296-9. Stem Cell Rev Rep. 2012. PMID: 21732091 Review.
References
-
- Orlic D, Kajstura J, Chimenti S, et al. Bone marrow cells regenerate infarcted myocardium. Nature. 2001;410:701–5. - PubMed
-
- Li TS, Hayashi M, Ito H, et al. Regeneration of infarcted myocardium by intramyocardial implantation of ex-vivo trasforming growth factor-beta-programmed bone marrow stem cells. Circulation. 2005;111:2438–45. - PubMed
-
- Schaefer A, Meyer GP, Fuchs M, et al. Impact of intracoronary bone marrow cell transfer on diastolic function in patients after acute myocardial infarction: results from the BOOST trial. Eur Heart J. 2006;27:929–35. - PubMed
-
- Meyer GP, Wollert KC, Lotz J, et al. Intracoronary bone marrow cell transfer after myocardial infarction; eighteen months’ follow-up data from the randomized, controlled BOOST (Bone marrow transfer to enhance ST-elevation infarct regeneration) trial. Circulation. 2006;113:1287–94. - PubMed
-
- Lunde K, Solheim S, Aakhus R, et al. Intracoronary injection of mononuclear bone marrow cells in acute myocardial infarction. N Engl J Med. 2006;335:1199–209. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
