

Efficacy and tolerability of tocilizumab in rheumatoid arthritis patients seen in daily clinical practice in Japan: results from a retrospective study (REACTION study)
- PMID: 20953815
- PMCID: PMC3071926
- DOI: 10.1007/s10165-010-0366-7
Efficacy and tolerability of tocilizumab in rheumatoid arthritis patients seen in daily clinical practice in Japan: results from a retrospective study (REACTION study)
Abstract
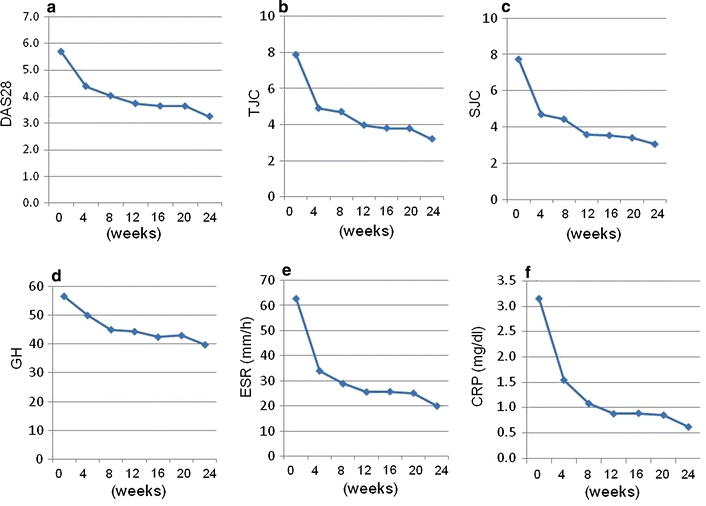
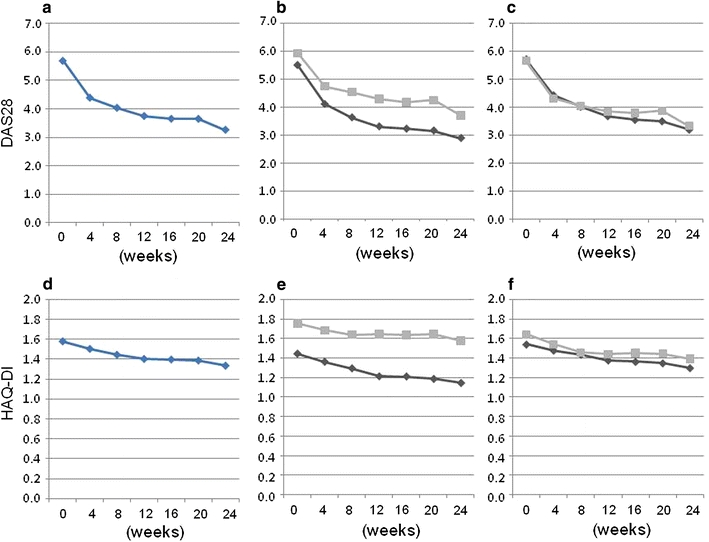
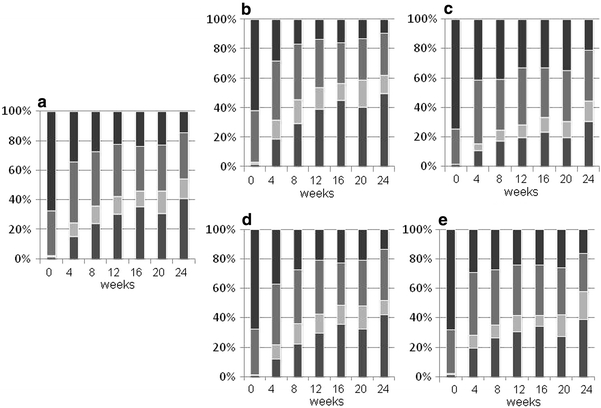
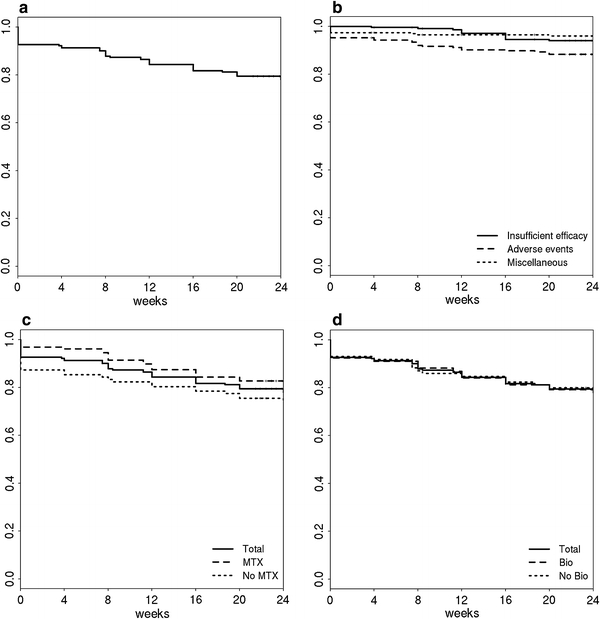
Tocilizumab, a humanized monoclonal antibody to the interleukin 6 (IL-6) receptor, was approved for use as rheumatoid arthritis (RA) therapy in Japan in 2008, but its efficacy and tolerability in daily practice has not yet been reported. We report the results of a multicenter retrospective study on the efficacy and safety of tocilizumab involving all patients (n = 229) who were started on tocilizumab therapy at three rheumatology institutes in Japan from April 2008 through to March 2009. Tocilizumab was infused every 4 weeks at a dose of 8 mg/kg according to the drug labeling. Among the 229 patients, 55% concomitantly received methotrexate (MTX) and 63% had previously received anti-tumor necrosis factor (TNF) therapy. Average disease activity score (DAS) 28 of all 229 patients significantly decreased from 5.70 to 3.25 after 24 weeks of therapy. A European League Against Rheumatism (EULAR) good response and DAS28 remission was achieved in 57.4 and 40.7% of the patients, respectively, at 24 weeks. White blood cell counts significantly decreased and liver enzymes and total cholesterol slightly but significantly increased; however, liver enzyme levels did not increase in patients without MTX. Tocilizumab was discontinued in 47 cases (20.5%) due to lack of efficacy (5.2%), adverse events (11.4%), and other reasons (3.9%). The overall retention rate at 24 weeks was 79.5%. Based on these results, we conclude that tocilizumab therapy in daily rheumatology practice appears to be highly efficacious and well tolerated among active RA patients, including the anti-TNF therapy-refractory population. Tocilizumab infusion is therefore applicable not only as an alternative approach for anti-TNF therapy-resistant patients, but also as primary biologic therapy for active RA patients.
Figures
Similar articles
-
Clinical, radiographic and functional effectiveness of tocilizumab for rheumatoid arthritis patients--REACTION 52-week study.Rheumatology (Oxford). 2011 Oct;50(10):1908-15. doi: 10.1093/rheumatology/ker221. Epub 2011 Jul 13. Rheumatology (Oxford). 2011. PMID: 21752873 Free PMC article.
-
Double-blind randomized controlled clinical trial of the interleukin-6 receptor antagonist, tocilizumab, in European patients with rheumatoid arthritis who had an incomplete response to methotrexate.Arthritis Rheum. 2006 Sep;54(9):2817-29. doi: 10.1002/art.22033. Arthritis Rheum. 2006. PMID: 16947782 Clinical Trial.
-
Retrospective clinical study on the notable efficacy and related factors of infliximab therapy in a rheumatoid arthritis management group in Japan: one-year clinical outcomes (RECONFIRM-2).Mod Rheumatol. 2008;18(2):146-52. doi: 10.1007/s10165-008-0026-3. Epub 2008 Feb 19. Mod Rheumatol. 2008. PMID: 18283523 Free PMC article.
-
Tocilizumab for rheumatoid arthritis.Cochrane Database Syst Rev. 2010 Jul 7;(7):CD008331. doi: 10.1002/14651858.CD008331.pub2. Cochrane Database Syst Rev. 2010. PMID: 20614469 Review.
-
Adalimumab, etanercept, infliximab, certolizumab pegol, golimumab, tocilizumab and abatacept for the treatment of rheumatoid arthritis not previously treated with disease-modifying antirheumatic drugs and after the failure of conventional disease-modifying antirheumatic drugs only: systematic review and economic evaluation.Health Technol Assess. 2016 Apr;20(35):1-610. doi: 10.3310/hta20350. Health Technol Assess. 2016. PMID: 27140438 Free PMC article. Review.
Cited by
-
Safety and efficacy of tocilizumab for the treatment of rheumatoid arthritis.Clin Med Insights Arthritis Musculoskelet Disord. 2012;5:27-42. doi: 10.4137/CMAMD.S7371. Epub 2012 Mar 5. Clin Med Insights Arthritis Musculoskelet Disord. 2012. PMID: 22438671 Free PMC article.
-
Tocilizumab, a humanized anti-interleukin-6 receptor antibody, for treatment of rheumatoid arthritis.Open Access Rheumatol. 2011 Feb 25;3:19-29. doi: 10.2147/OARRR.S17118. eCollection 2011. Open Access Rheumatol. 2011. PMID: 27790001 Free PMC article. Review.
-
Predictive factors of response to biological disease modifying antirheumatic drugs: towards personalized medicine.Mediators Inflamm. 2014;2014:386148. doi: 10.1155/2014/386148. Epub 2014 Jan 12. Mediators Inflamm. 2014. PMID: 24523570 Free PMC article. Review.
-
Interleukin 6 and rheumatoid arthritis.Biomed Res Int. 2014;2014:698313. doi: 10.1155/2014/698313. Epub 2014 Jan 12. Biomed Res Int. 2014. PMID: 24524085 Free PMC article. Review.
-
Tocilizumab for the treatment of rheumatoid arthritis and other systemic autoimmune diseases: current perspectives and future directions.Int J Rheumatol. 2012;2012:946048. doi: 10.1155/2012/946048. Epub 2012 Jan 18. Int J Rheumatol. 2012. PMID: 22315615 Free PMC article.
References
-
- Weaver AL. The impact of new biologicals in the treatment of rheumatoid arthritis. Rheumatology (Oxford) 2004;43[Suppl 3]:17–23. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
