

HIV infection and risk for incident pulmonary diseases in the combination antiretroviral therapy era
- PMID: 20851926
- PMCID: PMC3266024
- DOI: 10.1164/rccm.201006-0836OC
HIV infection and risk for incident pulmonary diseases in the combination antiretroviral therapy era
Abstract
Rationale: In aging HIV-infected populations comorbid diseases are important determinants of morbidity and mortality. Pulmonary diseases have not been systematically assessed in the combination antiretroviral therapy (ART) era.
Objectives: To determine the incidence of pulmonary diseases in HIV-infected persons compared with HIV-uninfected persons.
Methods: We analyzed data from the Veterans Aging Cohort Study Virtual Cohort, consisting of 33,420 HIV-infected veterans and 66,840 age, sex, race and ethnicity, and site-matched HIV-uninfected veterans. Using Poisson regression, incidence rates and adjusted incidence rate ratios were calculated to determine the association of HIV with pulmonary disease. The Virtual Cohort was merged with the 1999 Veterans Large Health Survey to adjust for self-reported smoking in a nested sample (14%).
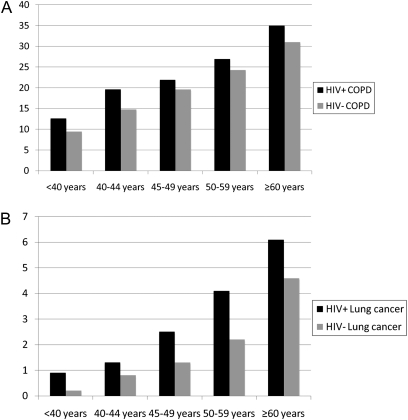
Measurements and main results: Incident chronic obstructive pulmonary disease, lung cancer, pulmonary hypertension, and pulmonary fibrosis, as well as pulmonary infections, were significantly more likely among HIV-infected patients compared with uninfected patients in adjusted analyses, although rates of asthma did not differ by HIV status. Bacterial pneumonia and chronic obstructive pulmonary disease were the two most common incident pulmonary diseases, whereas opportunistic pneumonias were less common. Absolute rates of most pulmonary diseases increased with age, although the relative differences between those with and without HIV infection were greatest in younger persons. Chronic obstructive pulmonary disease and asthma, as well as pulmonary infections, were less likely in those with lower HIV RNA levels and use of ART at baseline.
Conclusions: Pulmonary diseases among HIV-infected patients receiving care within the Veterans Affairs Healthcare System in the combination ART era reflect a substantial burden of non-AIDS-defining and chronic conditions, many of which are associated with aging.
Figures

Comment in
-
Risk and incidence of pulmonary diseases among HIV-infected patients in the era of combination antiretroviral therapy.Am J Respir Crit Care Med. 2011 Nov 1;184(9):1086-7; author reply 1087. doi: 10.1164/ajrccm.184.9.1086b. Am J Respir Crit Care Med. 2011. PMID: 22045750 Free PMC article. No abstract available.
Similar articles
-
Pulmonary symptoms and diagnoses are associated with HIV in the MACS and WIHS cohorts.BMC Pulm Med. 2014 Apr 30;14:75. doi: 10.1186/1471-2466-14-75. BMC Pulm Med. 2014. PMID: 24884738 Free PMC article.
-
HIV as an independent risk factor for incident lung cancer.AIDS. 2012 May 15;26(8):1017-25. doi: 10.1097/QAD.0b013e328352d1ad. AIDS. 2012. PMID: 22382152 Free PMC article.
-
Increased Echocardiographic Pulmonary Pressure in HIV-infected and -uninfected Individuals in the Veterans Aging Cohort Study.Am J Respir Crit Care Med. 2018 Apr 1;197(7):923-932. doi: 10.1164/rccm.201708-1555OC. Am J Respir Crit Care Med. 2018. PMID: 29131651 Free PMC article.
-
Pathogenesis of HIV and the lung.Curr HIV/AIDS Rep. 2013 Mar;10(1):42-50. doi: 10.1007/s11904-012-0140-x. Curr HIV/AIDS Rep. 2013. PMID: 23079728 Free PMC article. Review.
-
Obstructive Lung Diseases in HIV: A Clinical Review and Identification of Key Future Research Needs.Semin Respir Crit Care Med. 2016 Apr;37(2):277-88. doi: 10.1055/s-0036-1578801. Epub 2016 Mar 14. Semin Respir Crit Care Med. 2016. PMID: 26974304 Free PMC article. Review.
Cited by
-
Bronchiectasis and other chronic lung diseases in adolescents living with HIV.Curr Opin Infect Dis. 2017 Feb;30(1):21-30. doi: 10.1097/QCO.0000000000000325. Curr Opin Infect Dis. 2017. PMID: 27753690 Free PMC article. Review.
-
HIV and asthma, is there an association?Respir Med. 2012 Apr;106(4):493-9. doi: 10.1016/j.rmed.2011.12.017. Epub 2012 Jan 27. Respir Med. 2012. PMID: 22285768 Free PMC article. Review.
-
Waiting to inhale: An exploratory review of conditions that may predispose to pulmonary hypertension and right heart failure in persons exposed to household air pollution in low- and middle-income countries.Glob Heart. 2012 Sep 1;7(3):249-259. doi: 10.1016/j.gheart.2012.06.015. Glob Heart. 2012. PMID: 23687634 Free PMC article.
-
Human immunodeficiency virus-associated obstructive lung diseases.Clin Chest Med. 2013 Jun;34(2):273-82. doi: 10.1016/j.ccm.2013.02.002. Epub 2013 Apr 8. Clin Chest Med. 2013. PMID: 23702176 Free PMC article. Review.
-
COPD in People with HIV: Epidemiology, Pathogenesis, Management, and Prevention Strategies.Int J Chron Obstruct Pulmon Dis. 2023 Nov 29;18:2795-2817. doi: 10.2147/COPD.S388142. eCollection 2023. Int J Chron Obstruct Pulmon Dis. 2023. PMID: 38050482 Free PMC article. Review.
References
-
- Rosen MJ, Clayton K, Schneider RF, Fulkerson W, Rao AV, Stansell J, Kvale PA, Glassroth J, Reichman LB, Wallace JM, et al. Intensive care of patients with HIV infection: utilization, critical illnesses, and outcomes. Pulmonary Complications of HIV Infection Study Group. Am J Respir Crit Care Med 1997;155:67–71. - PubMed
-
- Murray JF, Mills J. Pulmonary infectious complications of human immunodeficiency virus infection. Part I. Am Rev Respir Dis 1990;141:1356–1372. - PubMed
-
- Wallace JM, Hansen NI, Lavange L, Glassroth J, Browdy BL, Rosen MJ, Kvale PA, Mangura BT, Reichman LB, Hopewell PC. Respiratory disease trends in the Pulmonary Complications of HIV Infection Study cohort. Pulmonary Complications of HIV Infection Study Group. Am J Respir Crit Care Med 1997;155:72–80. - PubMed
-
- Diaz PT, King MA, Pacht ER, Wewers MD, Gadek JE, Nagaraja HN, Drake J, Clanton TL. Increased susceptibility to pulmonary emphysema among HIV-seropositive smokers. Ann Intern Med 2000;132:369–372. - PubMed
-
- Crothers K, Butt AA, Gibert CL, Rodriguez-Barradas MC, Crystal S, Justice AC. Increased COPD among HIV-positive compared to HIV-negative veterans. Chest 2006;130:1326–1333. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
