

Pharmacotherapy for prevention and treatment of acute respiratory distress syndrome: current and experimental approaches
- PMID: 20568833
- PMCID: PMC7100688
- DOI: 10.2165/10898570-000000000-00000
Pharmacotherapy for prevention and treatment of acute respiratory distress syndrome: current and experimental approaches
Abstract
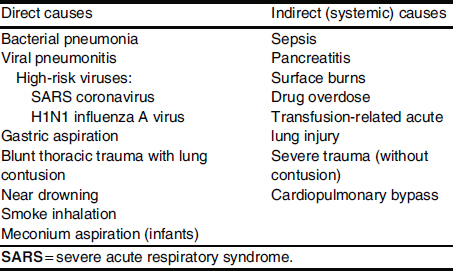
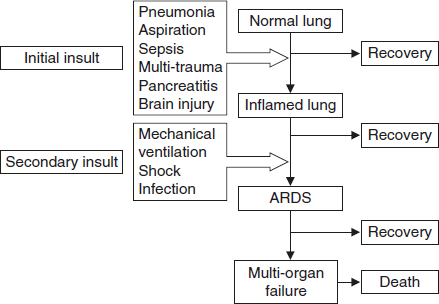
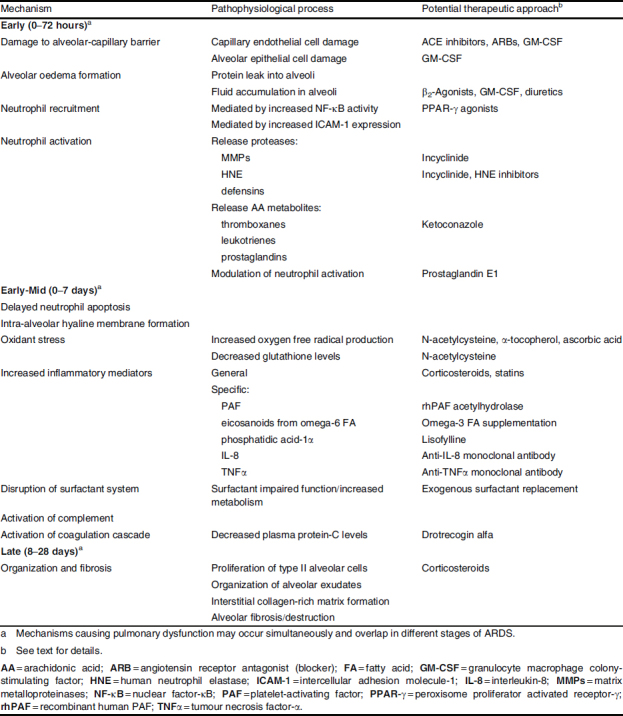
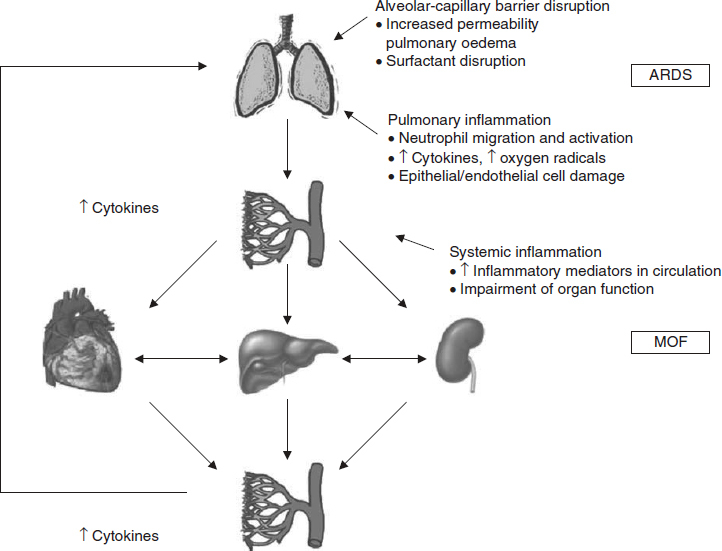
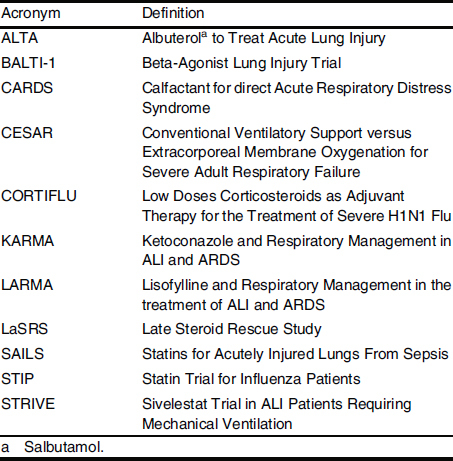
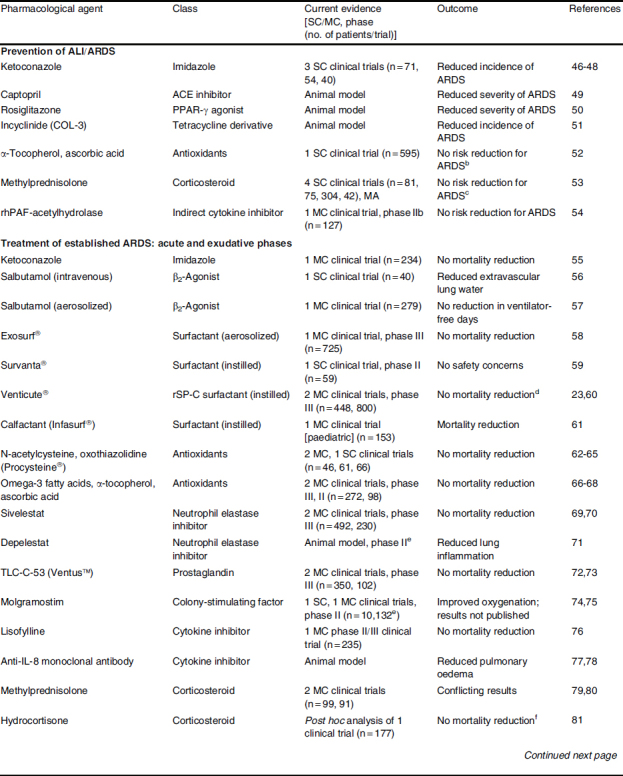
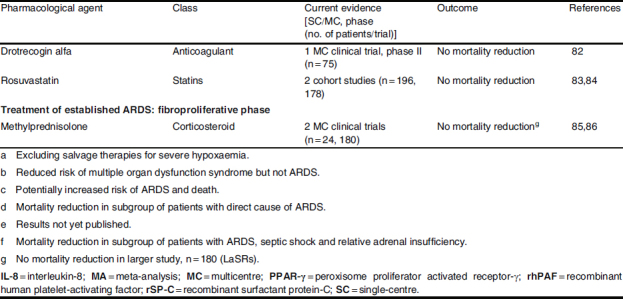
The acute respiratory distress syndrome (ARDS) arises from direct and indirect injury to the lungs and results in a life-threatening form of respiratory failure in a heterogeneous, critically ill patient population. Critical care technologies used to support patients with ARDS, including strategies for mechanical ventilation, have resulted in improved outcomes in the last decade. However, there is still a need for effective pharmacotherapies to treat ARDS, as mortality rates remain high. To date, no single pharmacotherapy has proven effective in decreasing mortality in adult patients with ARDS, although exogenous surfactant replacement has been shown to reduce mortality in the paediatric population with ARDS from direct causes. Several promising therapies are currently being investigated in preclinical and clinical trials for treatment of ARDS in its acute and subacute, exudative phases. These include exogenous surfactant therapy, beta(2)-adrenergic receptor agonists, antioxidants, immunomodulating agents and HMG-CoA reductase inhibitors (statins). Recent research has also focused on prevention of acute lung injury and acute respiratory distress in patients at risk. Drugs such as captopril, rosiglitazone and incyclinide (COL-3), a tetracycline derivative, have shown promising results in animal models, but have not yet been tested clinically. Further research is needed to discover therapies to treat ARDS in its late, fibroproliferative phase. Given the vast number of negative clinical trials to date, it is unlikely that a single pharmacotherapy will effectively treat all patients with ARDS from differing causes. Future randomized controlled trials should target specific, more homogeneous subgroups of patients for single or combination therapy.
Figures
Similar articles
-
Pharmacotherapy of acute lung injury and the acute respiratory distress syndrome.J Intensive Care Med. 2006 May-Jun;21(3):119-43. doi: 10.1177/0885066606287045. J Intensive Care Med. 2006. PMID: 16672636 Free PMC article. Review.
-
Pharmacological management of adult patients with acute respiratory distress syndrome.Expert Opin Pharmacother. 2020 Dec;21(17):2169-2183. doi: 10.1080/14656566.2020.1801636. Epub 2020 Aug 12. Expert Opin Pharmacother. 2020. PMID: 32783481 Review.
-
Therapeutic iloprost for the treatment of acute respiratory distress syndrome (ARDS) (the ThIlo trial): a prospective, randomized, multicenter phase II study.Trials. 2020 Mar 4;21(1):242. doi: 10.1186/s13063-020-4163-0. Trials. 2020. PMID: 32131881 Free PMC article.
-
Evolution of treatments for patients with acute lung injury.Expert Opin Investig Drugs. 2005 May;14(5):633-45. doi: 10.1517/13543784.14.5.633. Expert Opin Investig Drugs. 2005. PMID: 15926869 Review.
-
Nanotherapeutics in the treatment of acute respiratory distress syndrome.Life Sci. 2021 Jul 1;276:119428. doi: 10.1016/j.lfs.2021.119428. Epub 2021 Mar 27. Life Sci. 2021. PMID: 33785346 Free PMC article. Review.
Cited by
-
The effect of diet-induced serum hypercholesterolemia on the surfactant system and the development of lung injury.Biochem Biophys Rep. 2016 Sep;7:180-187. doi: 10.1016/j.bbrep.2016.06.009. Epub 2016 Jun 8. Biochem Biophys Rep. 2016. PMID: 28758151 Free PMC article.
-
Antioxidants and micronutrient supplementation in trauma patients.Curr Opin Clin Nutr Metab Care. 2012 Mar;15(2):181-7. doi: 10.1097/MCO.0b013e32835076df. Curr Opin Clin Nutr Metab Care. 2012. PMID: 22261953 Free PMC article. Review.
-
Network-Based Analysis of Fatal Comorbidities of COVID-19 and Potential Therapeutics.IEEE/ACM Trans Comput Biol Bioinform. 2021 Jul-Aug;18(4):1271-1280. doi: 10.1109/TCBB.2021.3075299. Epub 2021 Aug 6. IEEE/ACM Trans Comput Biol Bioinform. 2021. PMID: 33891554 Free PMC article.
-
CXCR4 receptor overexpression in mesenchymal stem cells facilitates treatment of acute lung injury in rats.J Biol Chem. 2015 Jan 23;290(4):1994-2006. doi: 10.1074/jbc.M114.605063. Epub 2014 Dec 9. J Biol Chem. 2015. PMID: 25492872 Free PMC article.
-
Protective effects of HY1702 on lipopolysaccharide-induced mild acute respiratory distress syndrome in mice.Eur J Pharmacol. 2020 Nov 15;887:173563. doi: 10.1016/j.ejphar.2020.173563. Epub 2020 Sep 16. Eur J Pharmacol. 2020. PMID: 32949601 Free PMC article.
References
-
- Bersten AD, Edibam C, Hunt T, et al. Incidence and mortality of acute lung injury and the acute respiratory distress syndrome in three Australian states. Am J Respir Crit Care Med. 2002;165(4):443–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
