

Markers of dysglycaemia and risk of coronary heart disease in people without diabetes: Reykjavik prospective study and systematic review
- PMID: 20520805
- PMCID: PMC2876150
- DOI: 10.1371/journal.pmed.1000278
Markers of dysglycaemia and risk of coronary heart disease in people without diabetes: Reykjavik prospective study and systematic review
Abstract
Background: Associations between circulating markers of dysglycaemia and coronary heart disease (CHD) risk in people without diabetes have not been reliably characterised. We report new data from a prospective study and a systematic review to help quantify these associations.
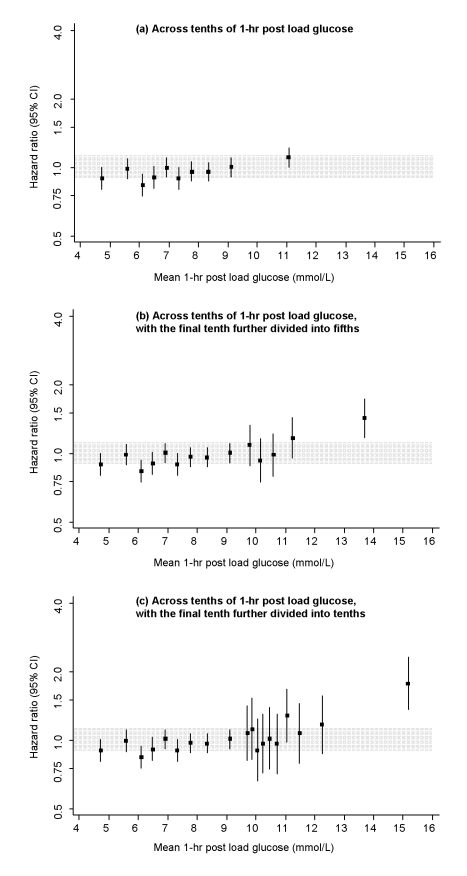
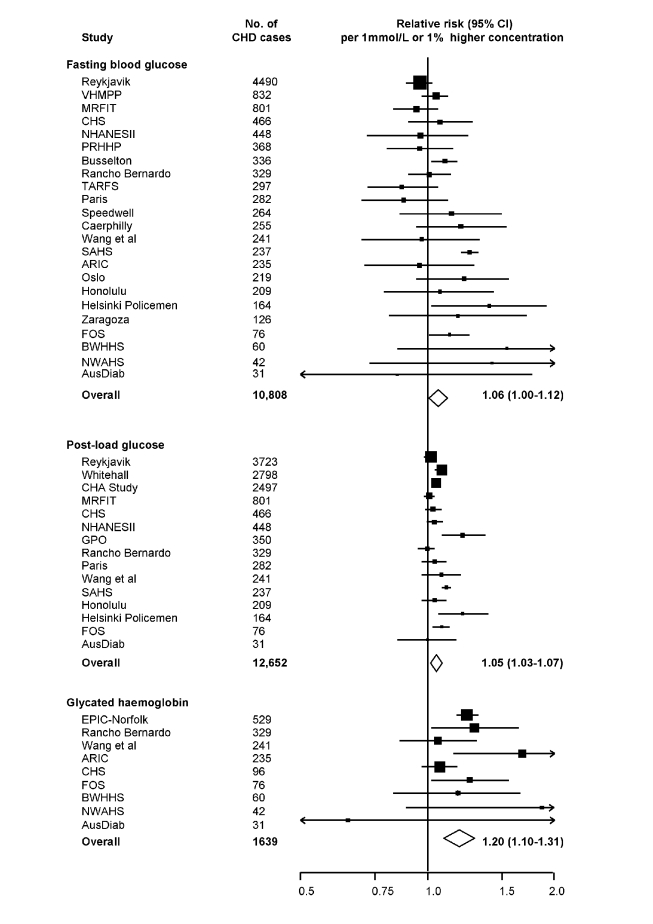
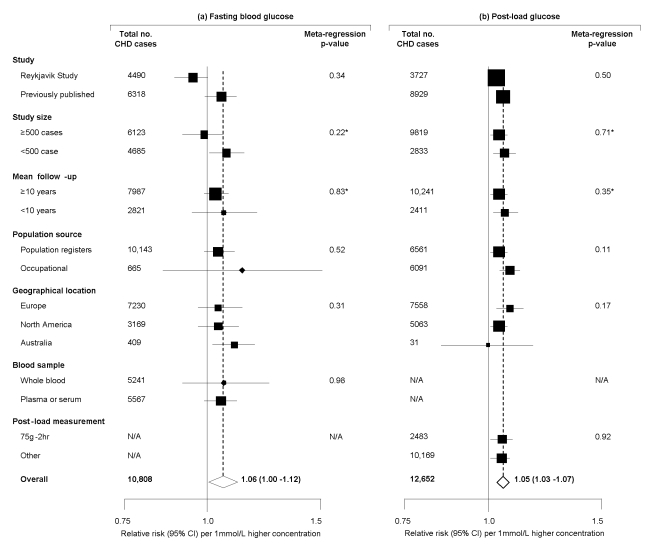
Methods and findings: Fasting and post-load glucose levels were measured in 18,569 participants in the population-based Reykjavik study, yielding 4,664 incident CHD outcomes during 23.5 y of mean follow-up. In people with no known history of diabetes at the baseline survey, the hazard ratio (HR) for CHD, adjusted for several conventional risk factors, was 2.37 (95% CI 1.79-3.14) in individuals with fasting glucose > or = 7.0 mmol/l compared to those < 7 mmol/l. At fasting glucose values below 7 mmol/l, adjusted HRs were 0.95 (0.89-1.01) per 1 mmol/l higher fasting glucose and 1.03 (1.01-1.05) per 1 mmol/l higher post-load glucose. HRs for CHD risk were generally modest and nonsignificant across tenths of glucose values below 7 mmol/l. We did a meta-analysis of 26 additional relevant prospective studies identified in a systematic review of Western cohort studies that recorded fasting glucose, post-load glucose, or glycated haemoglobin (HbA(1c)) levels. In this combined analysis, in which participants with a self-reported history of diabetes and/or fasting blood glucose > or = 7 mmol/l at baseline were excluded, relative risks for CHD, adjusted for several conventional risk factors, were: 1.06 (1.00-1.12) per 1 mmol/l higher fasting glucose (23 cohorts, 10,808 cases, 255,171 participants); 1.05 (1.03-1.07) per 1 mmol/l higher post-load glucose (15 cohorts, 12,652 cases, 102,382 participants); and 1.20 (1.10-1.31) per 1% higher HbA(1c) (9 cohorts, 1639 cases, 49,099 participants).
Conclusions: In the Reykjavik Study and a meta-analysis of other Western prospective studies, fasting and post-load glucose levels were modestly associated with CHD risk in people without diabetes. The meta-analysis suggested a somewhat stronger association between HbA(1c) levels and CHD risk.
Conflict of interest statement
JD has received research funding from the British Heart Foundation, BUPA Foundation, Denka, diaDexus, European Union, Evelyn Trust, GlaxoSmithKline MRC, Merck, National Heart, Lung, and Blood Institute, National Institute of Neurological Disorders and Stroke, Novartis, Pfizer, Roche, Wellcome Trust and UK Biobank. John Danesh is on the Editorial Board of </emph type="italic">PLoS Medicine</emph>.
Figures

Similar articles
-
Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies.Lancet. 2010 Jun 26;375(9733):2215-22. doi: 10.1016/S0140-6736(10)60484-9. Lancet. 2010. PMID: 20609967 Free PMC article.
-
Associations of alternative markers of glycemia with hemoglobin A(1c) and fasting glucose.Clin Chem. 2012 Dec;58(12):1648-55. doi: 10.1373/clinchem.2012.188367. Epub 2012 Sep 27. Clin Chem. 2012. PMID: 23019309 Free PMC article.
-
Cut-off values of fasting and post-load plasma glucose and HbA1c for predicting Type 2 diabetes in community-dwelling Japanese subjects: the Hisayama Study.Diabet Med. 2012 Jan;29(1):99-106. doi: 10.1111/j.1464-5491.2011.03378.x. Diabet Med. 2012. PMID: 21726278
-
The Effect of Dietary Glycaemic Index on Glycaemia in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Nutrients. 2018 Mar 19;10(3):373. doi: 10.3390/nu10030373. Nutrients. 2018. PMID: 29562676 Free PMC article. Review.
-
Association between glycated haemoglobin and the risk of congestive heart failure in diabetes mellitus: systematic review and meta-analysis.Eur J Heart Fail. 2013 Feb;15(2):185-93. doi: 10.1093/eurjhf/hfs156. Epub 2012 Oct 25. Eur J Heart Fail. 2013. PMID: 23099356 Review.
Cited by
-
The optimal cutoff value of glycated hemoglobin for detection of diabetic retinopathy.Diabetes Metab J. 2015 Feb;39(1):16-26. doi: 10.4093/dmj.2015.39.1.16. Diabetes Metab J. 2015. PMID: 25729708 Free PMC article. Review.
-
Do glycemic marker levels vary by race? Differing results from a cross-sectional analysis of individuals with and without diagnosed diabetes.BMJ Open Diabetes Res Care. 2016 Jun 10;4(1):e000213. doi: 10.1136/bmjdrc-2016-000213. eCollection 2016. BMJ Open Diabetes Res Care. 2016. PMID: 27335652 Free PMC article.
-
Prospectively Collected Cardiovascular Biomarkers and White Matter Hyperintensity Volume in Ischemic Stroke Patients.J Stroke Cerebrovasc Dis. 2020 May;29(5):104704. doi: 10.1016/j.jstrokecerebrovasdis.2020.104704. Epub 2020 Feb 22. J Stroke Cerebrovasc Dis. 2020. PMID: 32093989 Free PMC article.
-
New and emerging biomarkers in cardiovascular disease.Curr Diab Rep. 2015 Nov;15(11):88. doi: 10.1007/s11892-015-0661-y. Curr Diab Rep. 2015. PMID: 26370699 Review.
-
Increased cardiovascular disease, resource use, and costs before the clinical diagnosis of diabetes in veterans in the southeastern U.S.J Gen Intern Med. 2015 Jun;30(6):749-57. doi: 10.1007/s11606-014-3075-7. Epub 2015 Jan 22. J Gen Intern Med. 2015. PMID: 25608739 Free PMC article.
References
-
- Goldstein DE, Little RR, Lorenz RA, Malone JI, Nathan DM, et al. Tests of glycemia in diabetes. Diabetes Care. 2003;26(Suppl 1):S106–8. - PubMed
-
- Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. JAMA. 2002;287:2570–81. - PubMed
-
- Coutinho M, Gerstein HC, Wang Y, Yusuf S. The relationship between glucose and incident cardiovascular events. A metaregression analysis of published data from 20 studies of 95,783 individuals followed for 12.4 years. Diabetes Care. 1999;22:233–40. - PubMed
-
- Levitan EB, Song Y, Ford ES, Liu S. Is nondiabetic hyperglycemia a risk factor for cardiovascular disease? A meta-analysis of prospective studies. Arch Intern Med. 2004;164:2147–55. - PubMed
-
- DECODE Study Group, the European Diabetes Epidemiology Group. Glucose tolerance and cardiovascular mortality: comparison of fasting and 2-hour diagnostic criteria. Arch Intern Med. 2001;161:397–405. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
