

Precursor lesions of pancreatic cancer
- PMID: 20485640
- PMCID: PMC2871636
- DOI: 10.5009/gnl.2008.2.3.137
Precursor lesions of pancreatic cancer
Abstract
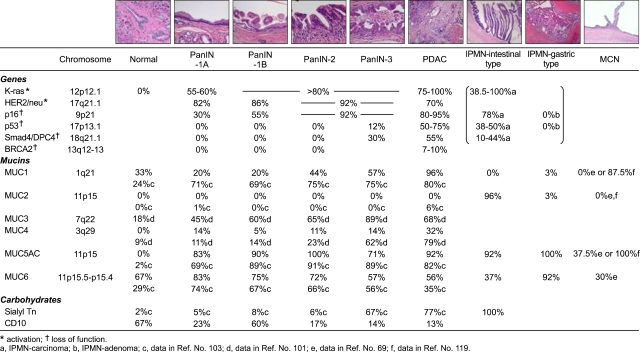
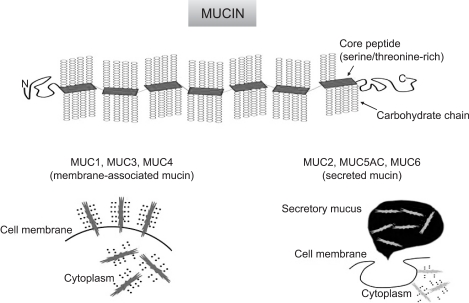
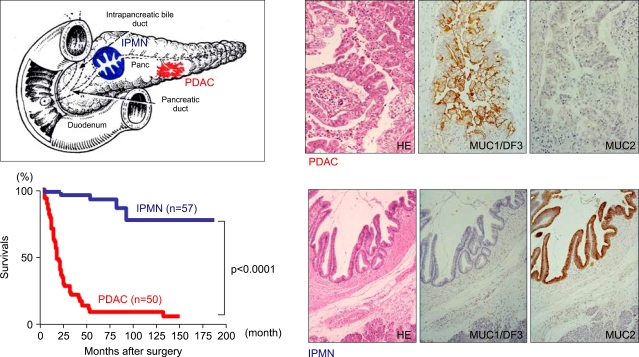
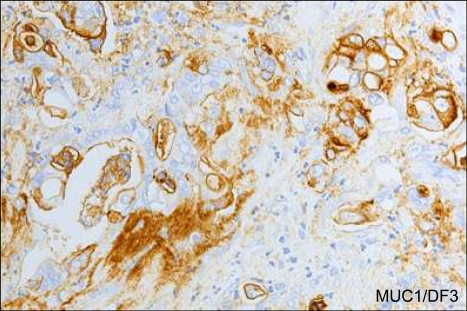
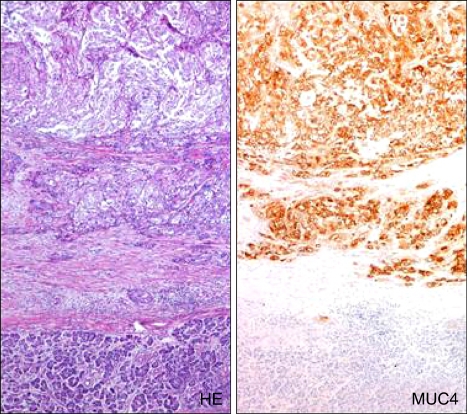
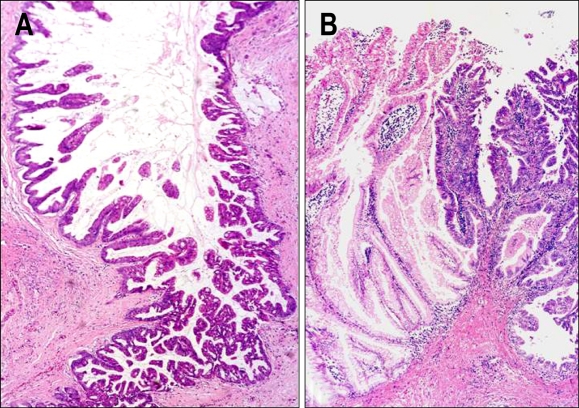
This review article describes morphological aspects, gene abnormalities, and mucin expression profiles in precursor lesions such as pancreatic intraepithelial neoplasia (PanIN), intraductal papillary mucinous neoplasm (IPMN), and mucinous cystic neoplasm (MCN) of the pancreas, as well as their relation to pancreatic ductal adenocarcinoma (PDAC). The gene abnormalities in precursors of PDAC are summarized as follows: (1) KRAS mutation and p16/CDKN2A inactivation are early events whose frequencies increase with the dysplasia grade in both PanIN and IPMN; (2) TP53 mutation and SMAD4/DPC4 inactivation are late events observed in PanIN3 or carcinomatous change of IPMN in both PanIN and IPMN, although the frequency of the TP53 mutation is lower in IPMN than in PDAC; and (3) also in MCN, KRAS mutation is an early event whose frequency increases with the dysplasia grade, whereas TP53 mutation and SMAD4/DPC4 inactivation are evident only in the carcinoma. The mucin expression profiles in precursors of PDAC are summarized as follows: (1) MUC1 expression increases with the PanIN grade, and is high in PDAC; (2) the expression pattern of MUC2 differs markedly between the major subtypes of IPMN with different malignancy potentials (i.e., IPMN-intestinal type with MUC2+ expression and IPMN-gastric type with MUC2- expression); (3) MUC2 is not expressed in any grade of PanINs, which is useful for differentiating PanIN from intestinal-type IPMN; (4) de novo expression of MUC4, which appears to increase with the dysplasia grade; and (5) high de novo expression of MUC5AC in all grades of PanINs, all types of IPMN, MCN, and PDAC.
Keywords: Gene analysis; Intraductal papillary mucinous neoplasm; Mucin expression; Mucinous cystic neoplasm; Pancreatic ductal adenocarcinoma; Pancreatic intraepithelial neoplasia.
Figures
Similar articles
-
Biological similarities and differences between pancreatic intraepithelial neoplasias and intraductal papillary mucinous neoplasms.Int J Gastrointest Cancer. 2005;35(2):111-9. doi: 10.1385/IJGC:35:2:111. Int J Gastrointest Cancer. 2005. PMID: 15879625
-
Loss of Trefoil Factor 2 From Pancreatic Duct Glands Promotes Formation of Intraductal Papillary Mucinous Neoplasms in Mice.Gastroenterology. 2016 Dec;151(6):1232-1244.e10. doi: 10.1053/j.gastro.2016.07.045. Epub 2016 Aug 12. Gastroenterology. 2016. PMID: 27523981 Free PMC article.
-
MUC2 expression and prevalence of high-grade dysplasia and invasive carcinoma in mixed-type intraductal papillary mucinous neoplasm of the pancreas.Pancreatology. 2013 Nov-Dec;13(6):583-8. doi: 10.1016/j.pan.2013.08.007. Epub 2013 Aug 30. Pancreatology. 2013. PMID: 24280573
-
Ductal neoplasia of the pancreas: nosologic, clinicopathologic, and biologic aspects.Semin Radiat Oncol. 2005 Oct;15(4):254-64. doi: 10.1016/j.semradonc.2005.04.001. Semin Radiat Oncol. 2005. PMID: 16183479 Review.
-
Mucins in neoplasms of pancreas, ampulla of Vater and biliary system.World J Gastrointest Oncol. 2016 Oct 15;8(10):725-734. doi: 10.4251/wjgo.v8.i10.725. World J Gastrointest Oncol. 2016. PMID: 27795812 Free PMC article. Review.
Cited by
-
The function of p97/valosin-containing protein (VCP) and small VCP-interacting protein (SVIP) in invasion and migration of pancreatic cancer cells.Turk J Med Sci. 2024 Jun 4;54(5):1154-1164. doi: 10.55730/1300-0144.5894. eCollection 2024. Turk J Med Sci. 2024. PMID: 39473740 Free PMC article.
-
Laser Capture Microdissection: A Gear for Pancreatic Cancer Research.Int J Mol Sci. 2022 Nov 23;23(23):14566. doi: 10.3390/ijms232314566. Int J Mol Sci. 2022. PMID: 36498893 Free PMC article. Review.
-
Peroxisome proliferator activated receptors at the crossroad of obesity, diabetes, and pancreatic cancer.World J Gastroenterol. 2016 Feb 28;22(8):2441-59. doi: 10.3748/wjg.v22.i8.2441. World J Gastroenterol. 2016. PMID: 26937133 Free PMC article. Review.
-
A concise review on the current understanding of pancreatic cancer stem cells.J Cancer Stem Cell Res. 2014;2:e1004. doi: 10.14343/jcscr.2014.2e1004. J Cancer Stem Cell Res. 2014. PMID: 26451384 Free PMC article.
-
Antagonism between Prdm16 and Smad4 specifies the trajectory and progression of pancreatic cancer.J Cell Biol. 2023 Apr 3;222(4):e202203036. doi: 10.1083/jcb.202203036. Epub 2023 Feb 24. J Cell Biol. 2023. PMID: 36828547 Free PMC article.
References
-
- Isaji S, Kawarada Y, Uemoto S. Classification of pancreatic cancer: comparison of Japanese and UICC classifications. Pancreas. 2004;28:231–234. - PubMed
-
- Hruban RH, Adsay NV, Albores-Saavedra J, et al. Pancreatic intraepithelial neoplasia: a new nomenclature and classification system for pancreatic duct lesions. Am J Surg Pathol. 2001;25:579–586. - PubMed
-
- Klöppel G, Hruban RH, Longnecker DS, et al. Tumours of the exocrine pancreas. In: Hamilton SR, Aaltonen LA, editors. Pathology and genetics of tumours of the digestive system, World Health Organization Classification of Tumours. Lyon: IARC Press; 2000. pp. 219–240.
-
- Hruban RJ, Pitman MB, Klimstra DS. AFIP Atlas of tumor pathology. Washington DC: American Registry of Pathology; 2007. Tumors of the pancreas. (Fourth series).
-
- Osako M, Yonezawa S, Siddiki B, et al. Immunohistochemical study of mucin carbohydrates and core proteins in human pancreatic tumors. Cancer. 1993;71:2191–2199. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
