

HPV-associated head and neck cancer: a virus-related cancer epidemic
- PMID: 20451455
- PMCID: PMC5242182
- DOI: 10.1016/S1470-2045(10)70017-6
HPV-associated head and neck cancer: a virus-related cancer epidemic
Abstract
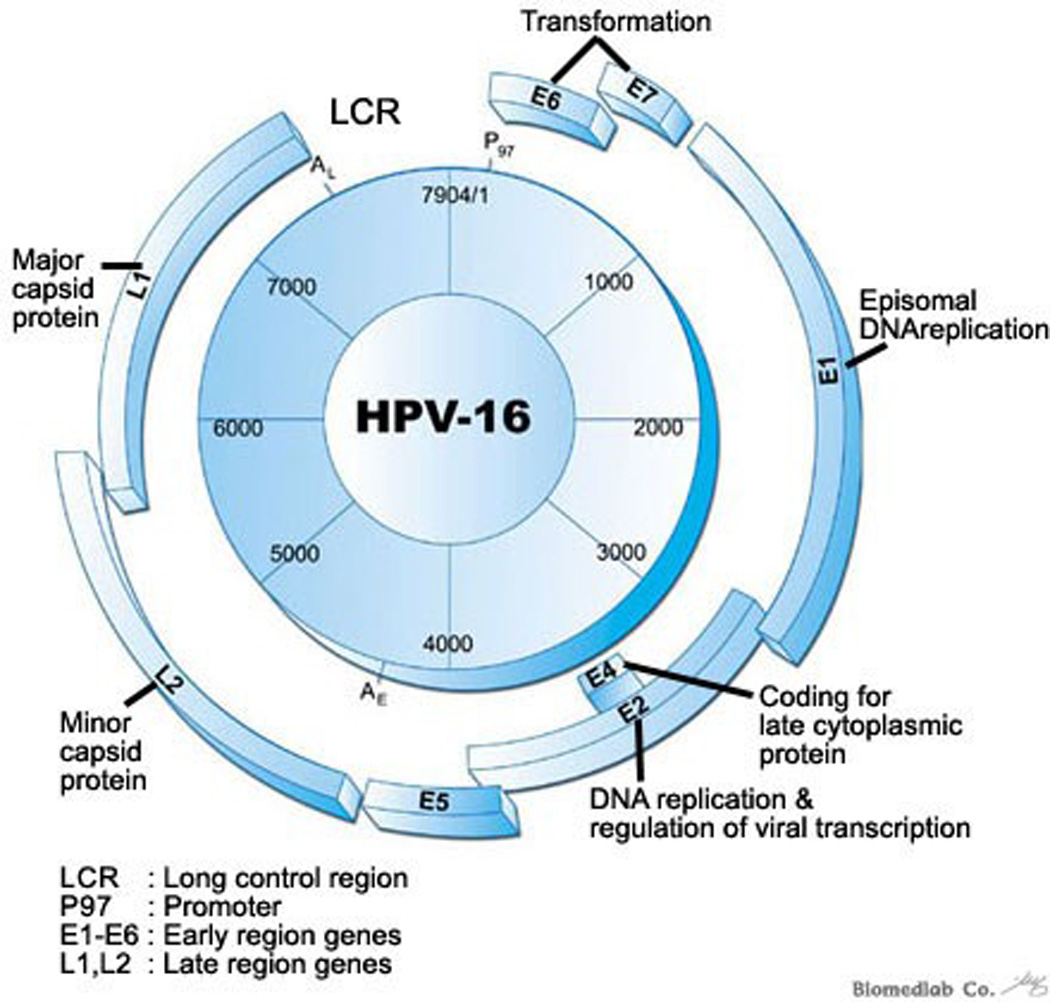
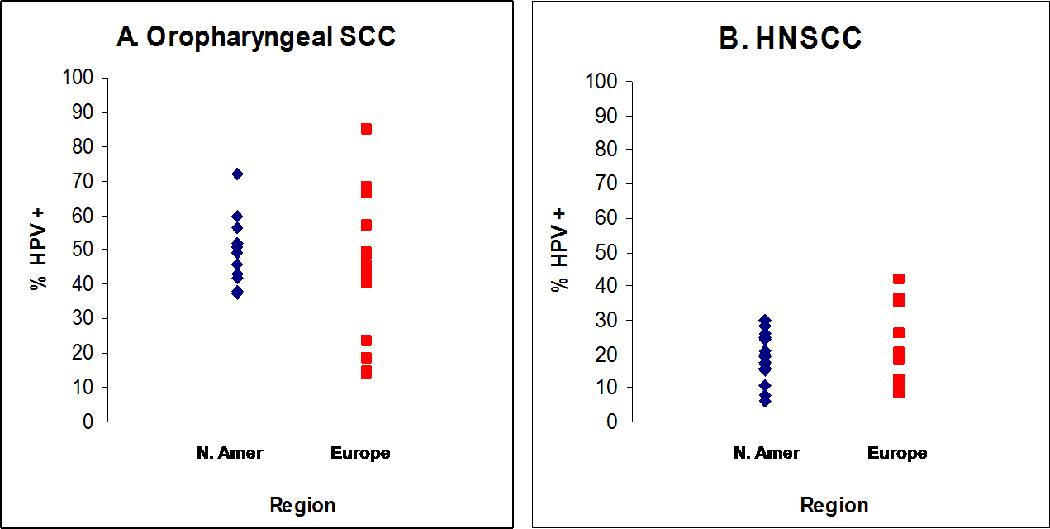
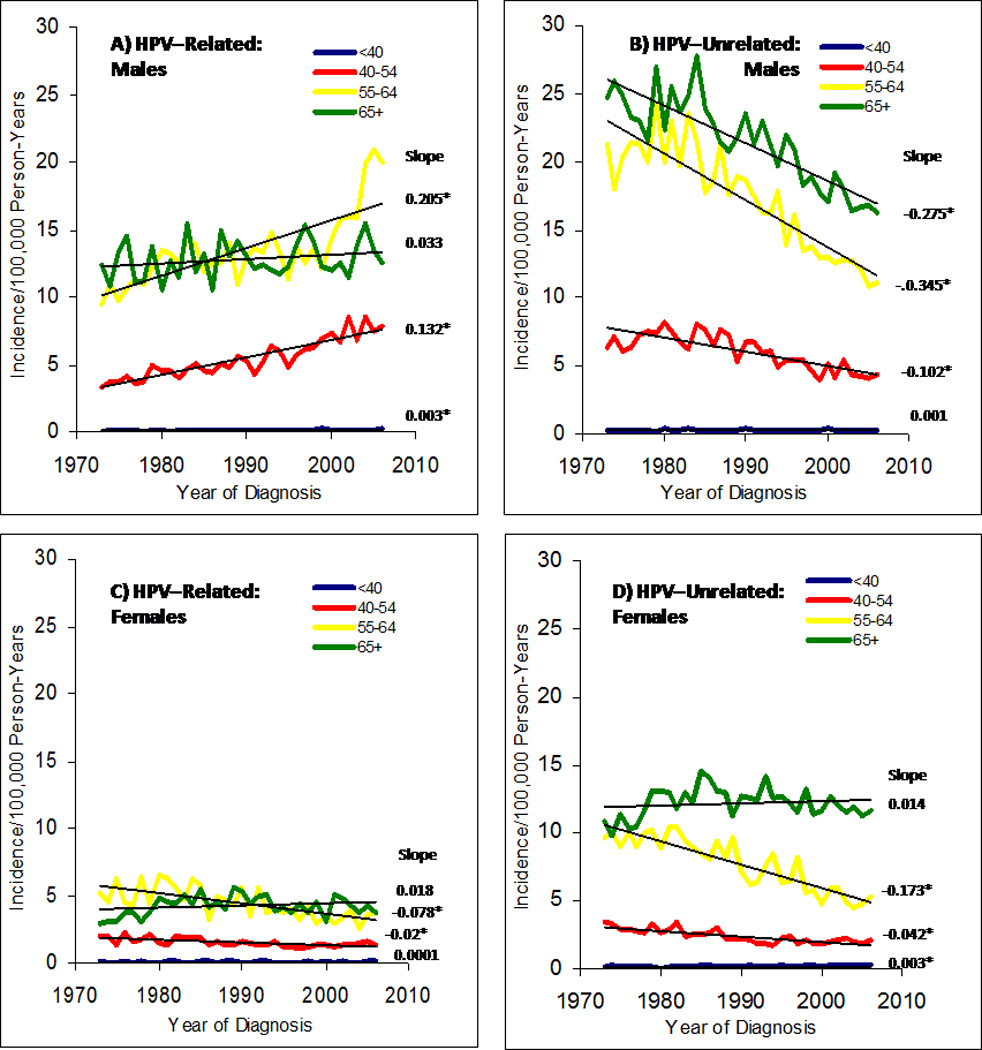
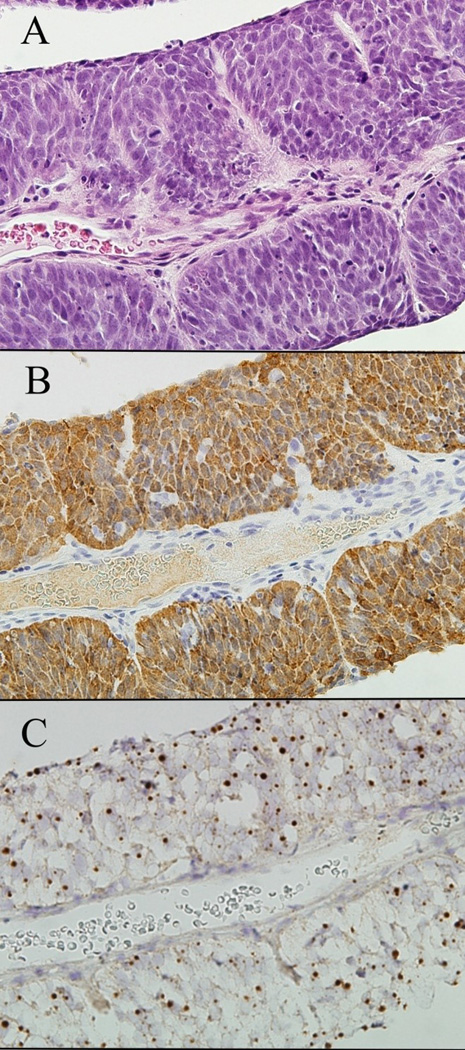
A rise in incidence of oropharyngeal squamous cell cancer--specifically of the lingual and palatine tonsils--in white men younger than age 50 years who have no history of alcohol or tobacco use has been recorded over the past decade. This malignant disease is associated with human papillomavirus (HPV) 16 infection. The biology of HPV-positive oropharyngeal cancer is distinct with P53 degradation, retinoblastoma RB pathway inactivation, and P16 upregulation. By contrast, tobacco-related oropharyngeal cancer is characterised by TP53 mutation and downregulation of CDKN2A (encoding P16). The best method to detect virus in tumour is controversial, and both in-situ hybridisation and PCR are commonly used; P16 immunohistochemistry could serve as a potential surrogate marker. HPV-positive oropharyngeal cancer seems to be more responsive to chemotherapy and radiation than HPV-negative disease. HPV 16 is a prognostic marker for enhanced overall and disease-free survival, but its use as a predictive marker has not yet been proven. Many questions about the natural history of oral HPV infection remain under investigation. For example, why does the increase in HPV-related oropharyngeal cancer dominate in men? What is the potential of HPV vaccines for primary prevention? Could an accurate method to detect HPV in tumour be developed? Which treatment strategies reduce toxic effects without compromising survival? Our aim with this review is to highlight current understanding of the epidemiology, biology, detection, and management of HPV-related oropharyngeal head and neck squamous cell carcinoma, and to describe unresolved issues.
2010 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declared not conflicts of interest.
Figures
Similar articles
-
HPV-positive head and neck tumours, a distinct clinical entity.B-ENT. 2015;11(2):81-7. B-ENT. 2015. PMID: 26563006 Review.
-
Human papillomavirus DNA detection in fine-needle aspirates as indicator of human papillomavirus-positive oropharyngeal squamous cell carcinoma: A prospective study.Head Neck. 2017 Mar;39(3):419-426. doi: 10.1002/hed.24641. Epub 2016 Nov 29. Head Neck. 2017. PMID: 27898186
-
The prognostic significance of the biomarker p16 in oropharyngeal squamous cell carcinoma.Clin Oncol (R Coll Radiol). 2013 Nov;25(11):630-8. doi: 10.1016/j.clon.2013.07.003. Epub 2013 Jul 31. Clin Oncol (R Coll Radiol). 2013. PMID: 23916365
-
Human papillomavirus as a marker of the natural history and response to therapy of head and neck squamous cell carcinoma.Semin Radiat Oncol. 2012 Apr;22(2):128-42. doi: 10.1016/j.semradonc.2011.12.004. Semin Radiat Oncol. 2012. PMID: 22385920 Review.
-
Molecular subclassification determined by human papillomavirus and epidermal growth factor receptor status is associated with the prognosis of oropharyngeal squamous cell carcinoma.Hum Pathol. 2016 Apr;50:51-61. doi: 10.1016/j.humpath.2015.11.001. Epub 2015 Nov 17. Hum Pathol. 2016. PMID: 26997438
Cited by
-
The cancer cell map initiative: defining the hallmark networks of cancer.Mol Cell. 2015 May 21;58(4):690-8. doi: 10.1016/j.molcel.2015.05.008. Mol Cell. 2015. PMID: 26000852 Free PMC article. Review.
-
Oropharyngeal cancer related to Human Papilloma Virus: incidence and prognosis in Madrid, Spain.Clin Transl Oncol. 2014 Mar;16(3):301-6. doi: 10.1007/s12094-013-1074-5. Epub 2013 Jul 5. Clin Transl Oncol. 2014. PMID: 23828503
-
The diagnostic and prognostic utility of insulin growth factor of squamous cell carcinoma in oral cavity.Tzu Chi Med J. 2020 Aug 25;33(2):160-164. doi: 10.4103/tcmj.tcmj_50_20. eCollection 2021 Apr-Jun. Tzu Chi Med J. 2020. PMID: 33912413 Free PMC article.
-
Sensitive MRD Detection from Lymphatic Fluid after Surgery in HPV-Associated Oropharyngeal Cancer.Clin Cancer Res. 2024 Apr 1;30(7):1409-1421. doi: 10.1158/1078-0432.CCR-23-1789. Clin Cancer Res. 2024. PMID: 37939112 Free PMC article.
-
HPV16 Down-Regulates the Insulin-Like Growth Factor Binding Protein 2 to Promote Epithelial Invasion in Organotypic Cultures.PLoS Pathog. 2015 Jun 24;11(6):e1004988. doi: 10.1371/journal.ppat.1004988. eCollection 2015 Jun. PLoS Pathog. 2015. PMID: 26107517 Free PMC article.
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55(2):74–108. - PubMed
-
- D'Souza G, Kreimer AR, Viscidi R, Pawlita M, Fakhry C, Koch WM, et al. Case-control study of human papillomavirus and oropharyngeal cancer. N Engl J Med. 2007;356(19):1944–1956. - PubMed
-
- Munoz N, Bosch FX, de Sanjose S, Herrero R, Castellsague X, Shah KV, et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med. 2003;348(6):518–527. - PubMed
-
- Kreimer AR, Clifford GM, Boyle P, Franceschi S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: a systematic review. Cancer Epidemiol Biomarkers Prev. 2005;14(2):467–475. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
