

HIV transmission risk through anal intercourse: systematic review, meta-analysis and implications for HIV prevention
- PMID: 20406794
- PMCID: PMC2929353
- DOI: 10.1093/ije/dyq057
HIV transmission risk through anal intercourse: systematic review, meta-analysis and implications for HIV prevention
Abstract
Background: The human immunodeficiency virus (HIV) infectiousness of anal intercourse (AI) has not been systematically reviewed, despite its role driving HIV epidemics among men who have sex with men (MSM) and its potential contribution to heterosexual spread. We assessed the per-act and per-partner HIV transmission risk from AI exposure for heterosexuals and MSM and its implications for HIV prevention.
Methods: Systematic review and meta-analysis of the literature on HIV-1 infectiousness through AI was conducted. PubMed was searched to September 2008. A binomial model explored the individual risk of HIV infection with and without highly active antiretroviral therapy (HAART).
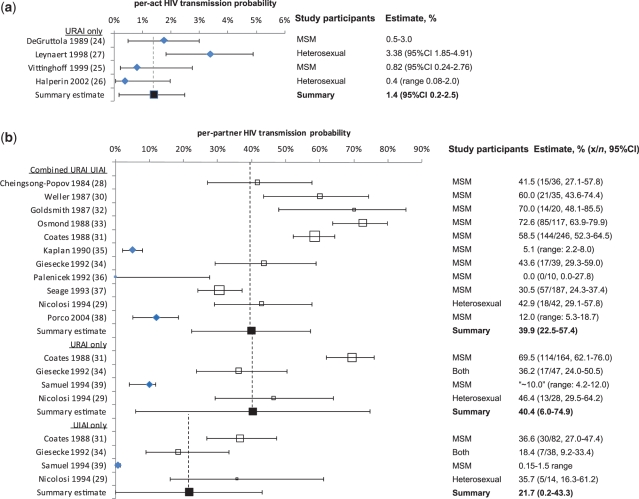
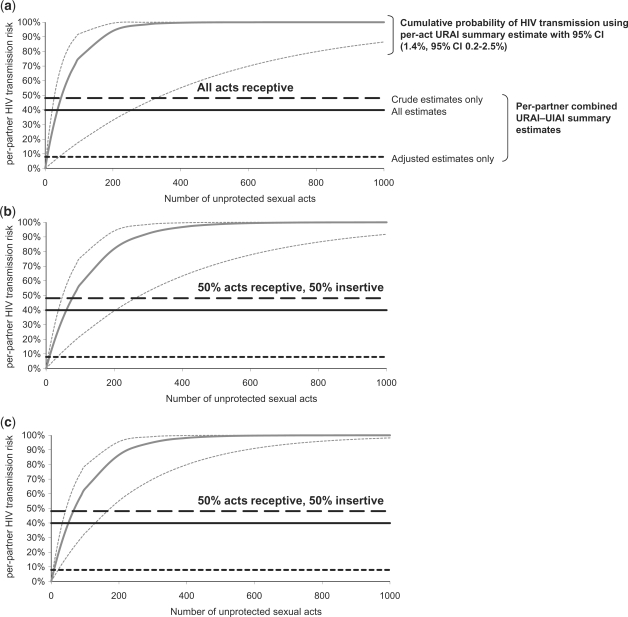
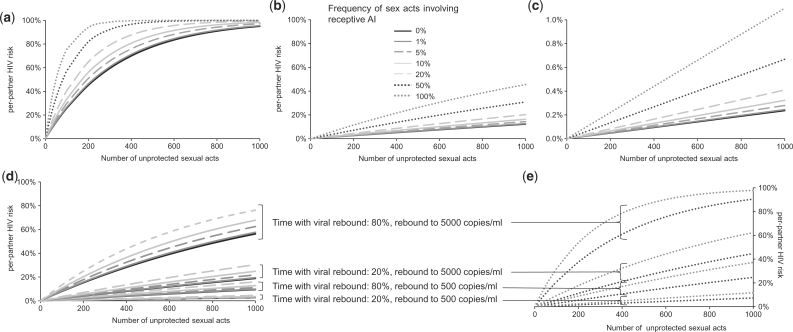
Results: A total of 62,643 titles were searched; four publications reporting per-act and 12 reporting per-partner transmission estimates were included. Overall, random effects model summary estimates were 1.4% [95% confidence interval (CI) 0.2-2.5)] and 40.4% (95% CI 6.0-74.9) for per-act and per-partner unprotected receptive AI (URAI), respectively. There was no significant difference between per-act risks of URAI for heterosexuals and MSM. Per-partner unprotected insertive AI (UIAI) and combined URAI-UIAI risk were 21.7% (95% CI 0.2-43.3) and 39.9% (95% CI 22.5-57.4), respectively, with no available per-act estimates. Per-partner combined URAI-UIAI summary estimates, which adjusted for additional exposures other than AI with a 'main' partner [7.9% (95% CI 1.2-14.5)], were lower than crude (unadjusted) estimates [48.1% (95% CI 35.3-60.8)]. Our modelling demonstrated that it would require unreasonably low numbers of AI HIV exposures per partnership to reconcile the summary per-act and per-partner estimates, suggesting considerable variability in AI infectiousness between and within partnerships over time. AI may substantially increase HIV transmission risk even if the infected partner is receiving HAART; however, predictions are highly sensitive to infectiousness assumptions based on viral load.
Conclusions: Unprotected AI is a high-risk practice for HIV transmission, probably with substantial variation in infectiousness. The significant heterogeneity between infectiousness estimates means that pooled AI HIV transmission probabilities should be used with caution. Recent reported rises in AI among heterosexuals suggest a greater understanding of the role AI plays in heterosexual sex lives may be increasingly important for HIV prevention.
Figures
Comment in
-
Commentary: probability of HIV transmission through anal intercourse.Int J Epidemiol. 2010 Aug;39(4):1064-5. doi: 10.1093/ije/dyq101. Epub 2010 May 28. Int J Epidemiol. 2010. PMID: 20511336 No abstract available.
Similar articles
-
Does per-act HIV-1 transmission risk through anal sex vary by gender? An updated systematic review and meta-analysis.Am J Reprod Immunol. 2018 Nov;80(5):e13039. doi: 10.1111/aji.13039. Epub 2018 Sep 2. Am J Reprod Immunol. 2018. PMID: 30175479 Free PMC article.
-
Unsafe Sexual Behavior Among Gay/Bisexual Men in the Era of Combination Antiretroviral Therapy (cART).AIDS Behav. 2017 Oct;21(10):2874-2885. doi: 10.1007/s10461-016-1614-4. AIDS Behav. 2017. PMID: 27990578 Free PMC article.
-
Sexual Activity Without Condoms and Risk of HIV Transmission in Serodifferent Couples When the HIV-Positive Partner Is Using Suppressive Antiretroviral Therapy.JAMA. 2016 Jul 12;316(2):171-81. doi: 10.1001/jama.2016.5148. JAMA. 2016. PMID: 27404185
-
Heterosexual risk of HIV transmission per sexual act under combined antiretroviral therapy: systematic review and bayesian modeling.Clin Infect Dis. 2014 Jul 1;59(1):115-22. doi: 10.1093/cid/ciu223. Epub 2014 Apr 9. Clin Infect Dis. 2014. PMID: 24723286 Free PMC article. Review.
-
Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men.Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001230. doi: 10.1002/14651858.CD001230.pub2. Cochrane Database Syst Rev. 2008. PMID: 18646068 Review.
Cited by
-
Enhanced Cohort Methods for HIV Research and Epidemiology (ENCORE): Protocol for a Nationwide Hybrid Cohort for Transgender Women in the United States.JMIR Res Protoc. 2024 Aug 27;13:e59846. doi: 10.2196/59846. JMIR Res Protoc. 2024. PMID: 39190916 Free PMC article.
-
Alcohol Use Disorder and HIV Risk in a National Survey of Men Who Have Sex with Men in Ukraine.Int J Behav Med. 2024 Jun 24. doi: 10.1007/s12529-024-10272-8. Online ahead of print. Int J Behav Med. 2024. PMID: 38914921
-
Dynamics and features of transmission clusters of HIV-1 subtypes in the state of São Paulo, Brazil.Front Public Health. 2024 Jun 5;12:1384512. doi: 10.3389/fpubh.2024.1384512. eCollection 2024. Front Public Health. 2024. PMID: 38903572 Free PMC article.
-
Herpes simplex virus spreads rapidly in human foreskin, partly driven by chemokine-induced redistribution of Nectin-1 on keratinocytes.PLoS Pathog. 2024 Jun 10;20(6):e1012267. doi: 10.1371/journal.ppat.1012267. eCollection 2024 Jun. PLoS Pathog. 2024. PMID: 38857290 Free PMC article.
-
Factors Associated with Sexually Transmitted Infections among Users of Voluntary HIV Counseling and Testing Centers in Portugal.Int J Sex Health. 2022 Feb 11;34(3):432-449. doi: 10.1080/19317611.2022.2032527. eCollection 2022. Int J Sex Health. 2022. PMID: 38596277 Free PMC article.
References
-
- Gisselquist D, Potterat JJ, Brody S. Running on empty: sexual co-factors are insufficient to fuel Africa’s turbocharged HIV epidemic. Int J STD AIDS. 2004;15:442–52. - PubMed
-
- Gisselquist D, Rothenberg R, Potterat J, Drucker E. HIV infections in sub-Saharan Africa not explained by sexual or vertical transmission. Int J STD AIDS. 2002;13:657–66. - PubMed
-
- Brody S, Potterat JJ. Assessing the role of anal intercourse in the epidemiology of AIDS in Africa. Int J STD AIDS. 2003;14:431–36. - PubMed
-
- Kloos H, Mariam DH. Some neglected and emerging factors in HIV transmission in Ethiopia. Ethiop Med J. 2007;45:103–7. - PubMed
-
- Smith LB, Adler NE, Tschann JM. Underreporting sensitive behaviors: the case of young women’s willingness to report abortion. Health Psychol. 1999;18:37–43. - PubMed
