

Diagnosis and screening of autosomal dominant polycystic kidney disease
- PMID: 20219617
- PMCID: PMC2841025
- DOI: 10.1053/j.ackd.2009.12.001
Diagnosis and screening of autosomal dominant polycystic kidney disease
Abstract
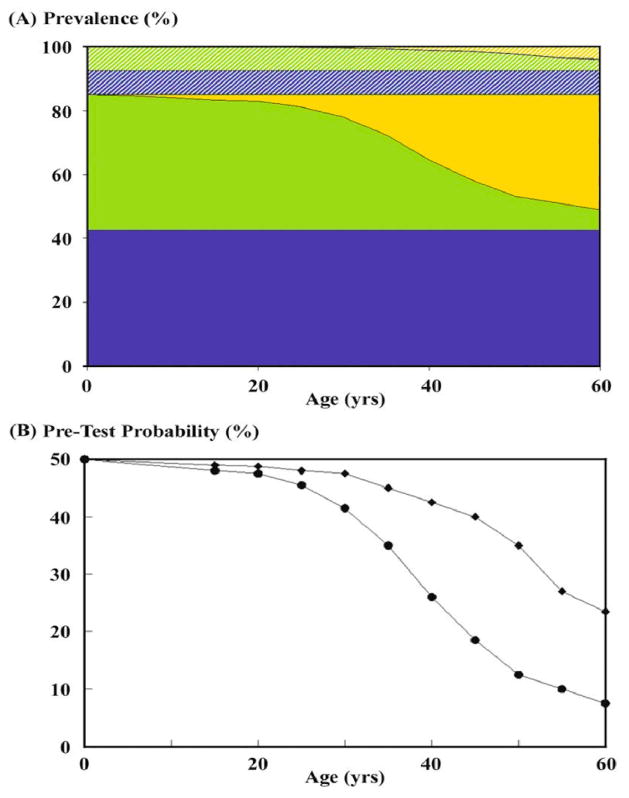
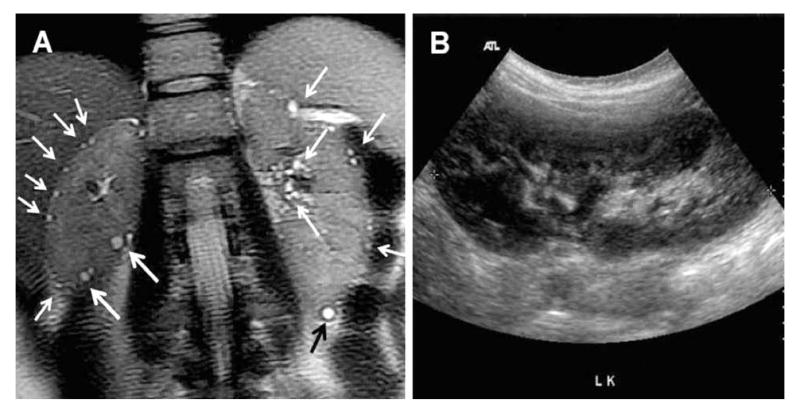
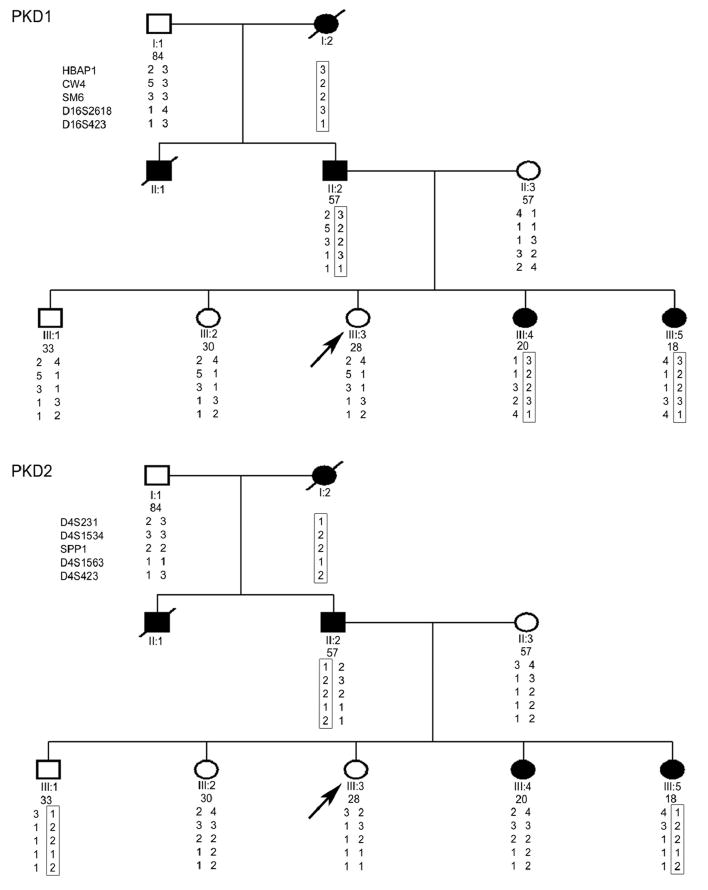
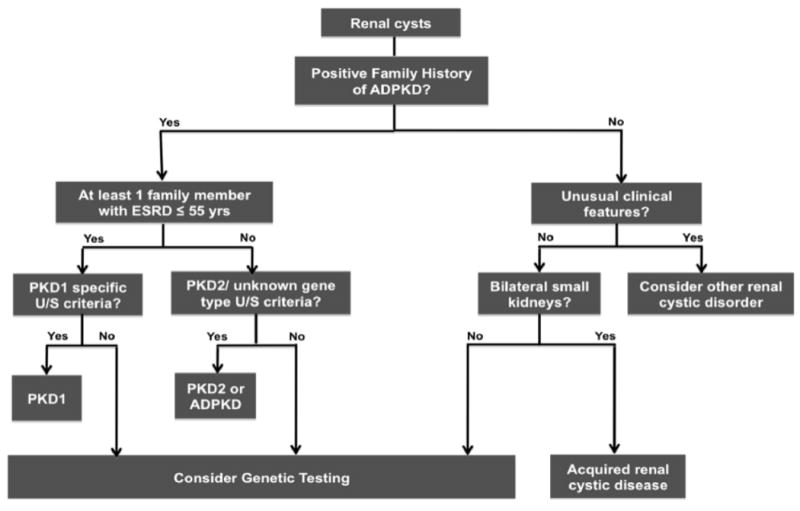
Autosomal dominant polycystic kidney disease (ADPKD) is the most common inherited cause of kidney failure and accounts for approximately 5% of ESRD population in the United States. The disorder is characterized by the focal and sporadic development of renal cysts, which increase in size and number with age. Mutations of PKD1 and PKD2 account for most of the cases. Although the clinical manifestations of both gene types overlap completely, PKD1 is associated with more severe disease than PKD2, with larger kidneys and earlier onset of ESRD. In general, renal ultrasonography is commonly used for the diagnosis of ADPKD, and age-dependent criteria have been defined for subjects at risk of PKD1. However, the utility of the PKD1 ultrasound criteria in the clinic setting is unclear because their performance characteristics have not been defined for the milder PKD2 and the gene type for most test subjects is unknown. Recently, highly predictive ultrasound diagnostic criteria have been derived for at-risk subjects of unknown gene type. Additionally, both DNA linkage or gene-based direct sequencing are now available for the diagnosis of ADPKD, especially in subjects with equivocal imaging results, subjects with a negative or indeterminate family history, or in younger at-risk individuals being evaluated as potential living-related kidney donors. Here, we review the clinical utilities and limitations of both imaging- and molecular-based diagnostic tests and outline our approach for the evaluation of individuals suspected to have ADPKD.
2010 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Practical genetics for autosomal dominant polycystic kidney disease.Nephron Clin Pract. 2011;118(1):c19-30. doi: 10.1159/000320887. Epub 2010 Nov 11. Nephron Clin Pract. 2011. PMID: 21071968 Review.
-
Diagnosis of autosomal-dominant polycystic kidney disease: an integrated approach.Semin Nephrol. 2010 Jul;30(4):356-65. doi: 10.1016/j.semnephrol.2010.06.002. Semin Nephrol. 2010. PMID: 20807608 Review.
-
Diagnostic approach in autosomal dominant polycystic kidney disease.Clin J Am Soc Nephrol. 2006 Sep;1(5):1108-14. doi: 10.2215/CJN.02190606. Epub 2006 Aug 9. Clin J Am Soc Nephrol. 2006. PMID: 17699332 Review.
-
PKD2-Related Autosomal Dominant Polycystic Kidney Disease: Prevalence, Clinical Presentation, Mutation Spectrum, and Prognosis.Am J Kidney Dis. 2017 Oct;70(4):476-485. doi: 10.1053/j.ajkd.2017.01.046. Epub 2017 Mar 27. Am J Kidney Dis. 2017. PMID: 28356211 Free PMC article.
-
Genetic testing in the assessment of living related kidney donors at risk of autosomal dominant polycystic kidney disease.Transplantation. 2015 May;99(5):1023-9. doi: 10.1097/TP.0000000000000466. Transplantation. 2015. PMID: 25340609
Cited by
-
Metabolomic profiling to identify early urinary biomarkers and metabolic pathway alterations in autosomal dominant polycystic kidney disease.Am J Physiol Renal Physiol. 2023 Jun 1;324(6):F590-F602. doi: 10.1152/ajprenal.00301.2022. Epub 2023 May 4. Am J Physiol Renal Physiol. 2023. PMID: 37141147 Free PMC article.
-
Genes Regulating Spermatogenesis and Sperm Function Associated With Rare Disorders.Front Cell Dev Biol. 2021 Feb 16;9:634536. doi: 10.3389/fcell.2021.634536. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 33665191 Free PMC article. Review.
-
Hereditary connective tissue diseases in young adult stroke: a comprehensive synthesis.Stroke Res Treat. 2011 Jan 20;2011:712903. doi: 10.4061/2011/712903. Stroke Res Treat. 2011. PMID: 21331163 Free PMC article.
-
Increasing extracellular matrix collagen level and MMP activity induces cyst development in polycystic kidney disease.BMC Nephrol. 2012 Sep 11;13:109. doi: 10.1186/1471-2369-13-109. BMC Nephrol. 2012. PMID: 22963260 Free PMC article.
-
Unique interstitial miRNA signature drives fibrosis in a murine model of autosomal dominant polycystic kidney disease.World J Nephrol. 2018 Sep 7;7(5):108-116. doi: 10.5527/wjn.v7.i5.108. World J Nephrol. 2018. PMID: 30211029 Free PMC article. Review.
References
-
- Gabow PA. Autosomal dominant polycystic kidney disease. N Engl J Med. 1993;329:332–342. - PubMed
-
- Iglesias CG, Torres VE, Offord KP, Holley KE, Beard CM, Kurland LT. Epidemiology of adult polycystic kidney disease, Olmsted County, Minnesota: 1935-1980. Am J Kidney Dis. 1983;2:630–639. - PubMed
-
- Davies F, Coles GA, Harper PS, Williams AJ, Evans C, Cochlin D. Polycystic kidney disease re-evaluated: a population-based study. Q J Med. 1991;79:477–485. - PubMed
-
- Peters DJ, Sandkuijl LA. Genetic heterogeneity of polycystic kidney disease in Europe. Contrib Nephrol. 1992;97:128–139. - PubMed
-
- Dobin A, Kimberling WJ, Pettinger W, Bailey-Wilson JE, Shugart YY, Gabow P. Segregation analysis of autosomal dominant polycystic kidney disease. Genet Epidemiol. 1993;10:189–200. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
