

Cholecalciferol supplementation in hemodialysis patients: effects on mineral metabolism, inflammation, and cardiac dimension parameters
- PMID: 20203163
- PMCID: PMC2863968
- DOI: 10.2215/CJN.06510909
Cholecalciferol supplementation in hemodialysis patients: effects on mineral metabolism, inflammation, and cardiac dimension parameters
Abstract
Background and objectives: Vitamin D deficiency is highly prevalent in chronic kidney disease. The aim of this study was to evaluate the effects of oral cholecalciferol supplementation on mineral metabolism, inflammation, and cardiac dimension parameters in long-term hemodialysis (HD) patients.
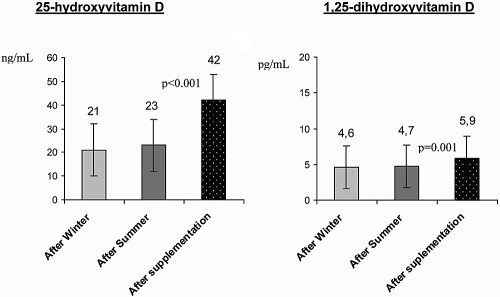
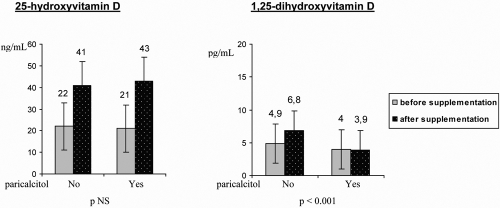
Design, setting, participants, & measurements: This 1-year prospective study included 158 HD patients. Serum levels of 25-hydroxyvitamin D [25(OH)D], 1,25-dihydroxyvitamin D [1,25(OH)(2)D], intact parathyroid hormone, and plasma brain natriuretic peptide as well as circulating bone metabolism and inflammation parameters were measured before and after supplementation. Baseline 25(OH)D and 1,25(OH)(2)D levels were measured twice (end of winter and of summer, respectively). Therapy with paricalcitol, sevelamer, and darbepoietin was evaluated.
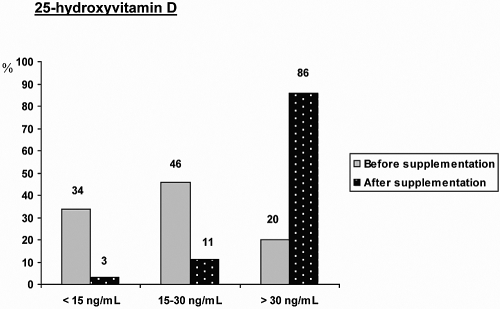
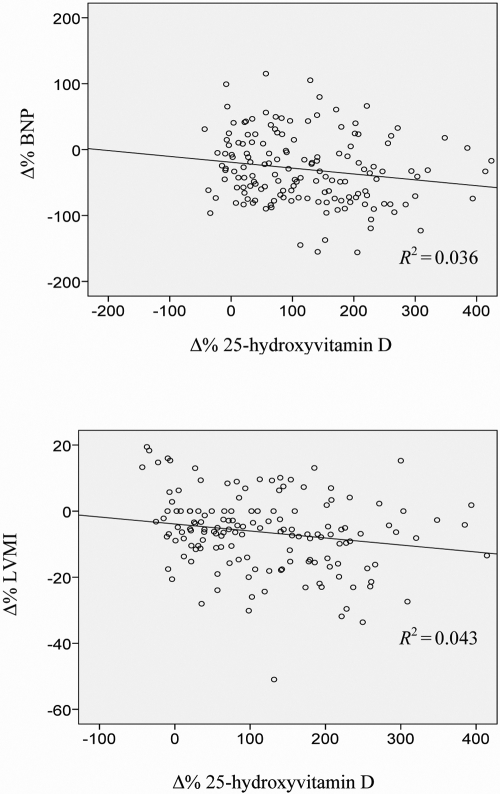
Results: There was an increase in serum 25(OH)D and 1,25(OH)(2)D levels after supplementation. Conversely, serum calcium, phosphorus, and intact parathyroid hormone were decreased. There was a reduction in the dosage and in the number of patients who were treated with paricalcitol and sevelamer. Darbepoietin use was also reduced, with no modification of hemoglobin values. Serum albumin increased and C-reactive protein decreased during the study. Brain natriuretic peptide levels and left ventricular mass index were significantly reduced at the end of the supplementation.
Conclusions: Oral cholecalciferol supplementation in HD patients seems to be an easy and cost-effective therapeutic measure. It allows reduction of vitamin D deficiency, better control of mineral metabolism with less use of active vitamin D, attenuation of inflammation, reduced dosing of erythropoiesis-stimulating agents, and possibly improvement of cardiac dysfunction.
Figures
Similar articles
-
Impact of cholecalciferol treatment on biomarkers of inflammation and myocardial structure in hemodialysis patients without hyperparathyroidism.J Ren Nutr. 2012 Mar;22(2):284-291. doi: 10.1053/j.jrn.2011.07.001. Epub 2011 Sep 10. J Ren Nutr. 2012. PMID: 21908203
-
Long-term cholecalciferol supplementation in hemodialysis patients: Effects on mineral metabolism, inflammation, and cardiac parameters.Semin Dial. 2023 Jan;36(1):29-36. doi: 10.1111/sdi.13066. Epub 2022 Mar 9. Semin Dial. 2023. PMID: 35262225
-
Low-dose cholecalciferol supplementation and dual vitamin D therapy in haemodialysis patients.Int Urol Nephrol. 2015 Jan;47(1):169-76. doi: 10.1007/s11255-014-0842-7. Epub 2014 Sep 28. Int Urol Nephrol. 2015. PMID: 25262147
-
Interventions for metabolic bone disease in children with chronic kidney disease.Cochrane Database Syst Rev. 2015 Nov 12;2015(11):CD008327. doi: 10.1002/14651858.CD008327.pub2. Cochrane Database Syst Rev. 2015. PMID: 26561037 Free PMC article. Review.
-
1alpha(OH)D3 One-alpha-hydroxy-cholecalciferol--an active vitamin D analog. Clinical studies on prophylaxis and treatment of secondary hyperparathyroidism in uremic patients on chronic dialysis.Dan Med Bull. 2008 Nov;55(4):186-210. Dan Med Bull. 2008. PMID: 19232159 Review.
Cited by
-
Integrated Proteomics and Metabolomics Analysis of Perirenal Adipose Tissue in Obese Rabbits Treated with a Restricted Diet.Biology (Basel). 2021 Apr 12;10(4):321. doi: 10.3390/biology10040321. Biology (Basel). 2021. PMID: 33921318 Free PMC article.
-
Seasonal variations in mortality and clinical indicators in international hemodialysis populations from the MONDO registry.BMC Nephrol. 2015 Aug 14;16:139. doi: 10.1186/s12882-015-0129-y. BMC Nephrol. 2015. PMID: 26272070 Free PMC article.
-
Vitamin D deficiency in hemodialysis patients.Indian J Endocrinol Metab. 2012 Mar;16(2):270-3. doi: 10.4103/2230-8210.93749. Indian J Endocrinol Metab. 2012. PMID: 22470866 Free PMC article.
-
Classical and emerging roles of vitamin D in hepatitis C virus infection.Semin Liver Dis. 2011 Nov;31(4):387-98. doi: 10.1055/s-0031-1297927. Epub 2011 Dec 21. Semin Liver Dis. 2011. PMID: 22189978 Free PMC article. Review.
-
Chronic Kidney Disease as a Risk Factor for Heart Failure With Preserved Ejection Fraction: A Focus on Microcirculatory Factors and Therapeutic Targets.Front Physiol. 2019 Sep 4;10:1108. doi: 10.3389/fphys.2019.01108. eCollection 2019. Front Physiol. 2019. PMID: 31551803 Free PMC article. Review.
References
-
- Gonzalez EA, Sachdeva A, Oliver DA, Martin KJ: Vitamin D insufficiency and deficiency in chronic kidney disease: A single center observational study. Am J Nephrol 24: 503– 510, 2004 - PubMed
-
- LaClair RE, Hellman RN, Karp SL, Kraus M, Ofner S, Li Q, Graves KL, Moe SM: Prevalence of calcidiol deficiency in CKD: A cross-sectional study across latitudes in the United States. Am J Kidney Dis 45: 1026– 1033, 2005 - PubMed
-
- Ishimura E, Nishizawa Y, Inaba M, Matsumoto N, Emoto M, Kawagishi T, Shoji S, Okuno S, Kim M, Miki T, Morii H: Serum levels of 1,25-dihydroxyvitamin D, 24,25-dihydroxyvitamin D, and 25-hydroxyvitamin D in nondialysed patients with chronic renal failure. Kidney Int 55: 1019– 1027, 1999 - PubMed
-
- Goodman WG, Coburn JW: The use of 1,25-dihydroxyvitamin D3 in early renal failure. Annu Rev Med 43: 227– 237, 1992 - PubMed
-
- Schroeder NJ, Cunningham J: What's new in vitamin D for the nephrologist? Nephrol Dial Transplant 15: 460– 466, 2000 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
