

Review
doi: 10.1002/hep.23478.
Now there are many (stages) where before there was one: In search of a pathophysiological classification of cirrhosis
Affiliations
- PMID: 20077563
- PMCID: PMC2882065
- DOI: 10.1002/hep.23478
Item in Clipboard
Review
Now there are many (stages) where before there was one: In search of a pathophysiological classification of cirrhosis
Hepatology.
2010 Apr.
No abstract available
Figures
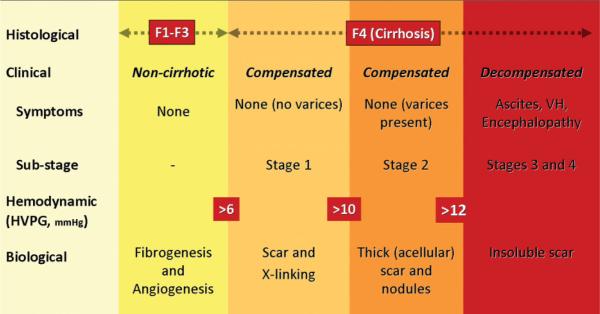
Classification of chronic liver disease based on histological, clinical, hemodynamic, and biological parameters. In the noncirrhotic stage (METAVIR F1–F3), there is no clinical evidence of cirrhosis, the HVPG is below 6 mmHg, and at this stage there is fibrogenesis and neovascularization. The cirrhotic stage (METAVIR F4) is broadly classified into two stages: compensated and decompensated, with clinical decompensation being defined by the development of ascites, variceal hemorrhage (VH), encephalopathy, and jaundice. Within the compensated stage, patients can be subclassified into those without varices (stage 1) and those with varices (stage 2). Those without varices can be further subclassified into those with an hepatic venous pressure gradient (HVPG) < or > 10 mmHg, which is the threshold pressure that predicts development of varices and decompensation. HVPG > 10 mmHg (clinically significant portal hypertension) correlates with thick scar and small nodules. In the decompensated stage, the scar is resistant to degradation. Complex circulatory (splanchnic and systemic) abnormalities that occur at this decompensated stage contribute to further decompensation, i.e., recurrent variceal hemorrhage, refractory ascites, and hepatorenal syndrome, and although HVPG retains prognostic value, other parameters that take into account liver insufficiency and a deranged circulatory state, such as the MELD score, are more predictive of death (not depicted in figure). Figure is modified from Friedman.
Comment in
-
Histological subclassification of cirrhosis.Hepatology. 2010 Aug;52(2):804-5. doi: 10.1002/hep.23655. Hepatology. 2010. PMID: 20593457 No abstract available.
Similar articles
-
[Physiopathology of liver cirrhosis in relation to the liver lesion].Nihon Naika Gakkai Zasshi. 1991 Oct 10;80(10):1568-71. Nihon Naika Gakkai Zasshi. 1991. PMID: 1774519 Japanese. No abstract available.
-
Cirrhosis: what else?Gastroenterol Clin Biol. 2010 Apr-May;34(4-5):252-4. doi: 10.1016/j.gcb.2010.03.007. Epub 2010 May 27. Gastroenterol Clin Biol. 2010. PMID: 20537484
-
Evaluation of rectal mucosal hemodynamics in patients with liver cirrhosis using reflectance spectrophotometry.Am J Gastroenterol. 1997 Jun;92(6):1022-5. Am J Gastroenterol. 1997. PMID: 9177523
-
[Child-Pugh classification in liver cirrhosis].Ryoikibetsu Shokogun Shirizu. 1995;(7):151-4. Ryoikibetsu Shokogun Shirizu. 1995. PMID: 8749441 Review. Japanese. No abstract available.
-
Cirrhosis of the liver: principles of classification, histogenesis, and pathogenesis.Pathol Annu. 1972;7:107-44. Pathol Annu. 1972. PMID: 4339775 Review. No abstract available.
Cited by
-
Where does TIPS fit in the management of patients with cirrhosis?JHEP Rep. 2020 May 23;2(4):100122. doi: 10.1016/j.jhepr.2020.100122. eCollection 2020 Aug. JHEP Rep. 2020. PMID: 32671331 Free PMC article. Review.
-
Portal hypertensive gastropathy as a prognostic index in patients with liver cirrhosis.BMC Gastroenterol. 2016 Aug 12;16(1):93. doi: 10.1186/s12876-016-0508-2. BMC Gastroenterol. 2016. PMID: 27519178 Free PMC article.
-
Short-term clinical outcomes of patients admitted with chronic liver disease to selected teaching hospitals in Ethiopia.PLoS One. 2019 Aug 30;14(8):e0221806. doi: 10.1371/journal.pone.0221806. eCollection 2019. PLoS One. 2019. PMID: 31469861 Free PMC article.
-
Beyond a broken heart: circulatory dysfunction in the failing Fontan.Pediatr Cardiol. 2014 Apr;35(4):569-79. doi: 10.1007/s00246-014-0881-y. Epub 2014 Feb 15. Pediatr Cardiol. 2014. PMID: 24531876 Review.
-
Clinical outcomes after treatment with direct antiviral agents: beyond the virological response in patients with previous HCV-related decompensated cirrhosis.BMC Infect Dis. 2022 Jan 27;22(1):94. doi: 10.1186/s12879-022-07076-0. BMC Infect Dis. 2022. PMID: 35086481 Free PMC article.
References
-
- Pinzani M, Rombouts K, Colagrande S. Fibrosis in chronic liver diseases: diagnosis and management. J Hepatol. 2005;42(Suppl. 1):S22–S36. - PubMed
-
- Poynard T, Bedossa P, Opolon P, the OBSVIRC MCADg Natural history of liver fibrosis progression in patients with chronic hepatitis C. Lancet. 1997;349:825–832. - PubMed
-
- Ishak K, Baptista A, Bianchi L, Callea F, De Groote J, Gudat F, et al. Histological grading and staging of chronic hepatitis. J Hepatol. 1995;22:696–699. - PubMed
-
- Knodell RG, Ishak KG, Black WC, Craig R, Kaplowitz N, Kiernan TW, et al. Formulation and application of a numerical scoring system for assessing histological activity in asymptomatic chronic active hepatitis. HEPATOLOGY. 1981;1:431–435. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical