

HIV-1 residual viremia correlates with persistent T-cell activation in poor immunological responders to combination antiretroviral therapy
- PMID: 19876401
- PMCID: PMC2765414
- DOI: 10.1371/journal.pone.0007658
HIV-1 residual viremia correlates with persistent T-cell activation in poor immunological responders to combination antiretroviral therapy
Abstract
Background: The clinical significance and cellular sources of residual human immunodeficiency virus type 1 (HIV-1) production despite suppressive combination antiretroviral therapy (cART) remain unclear and the effect of low-level viremia on T-cell homeostasis is still debated.
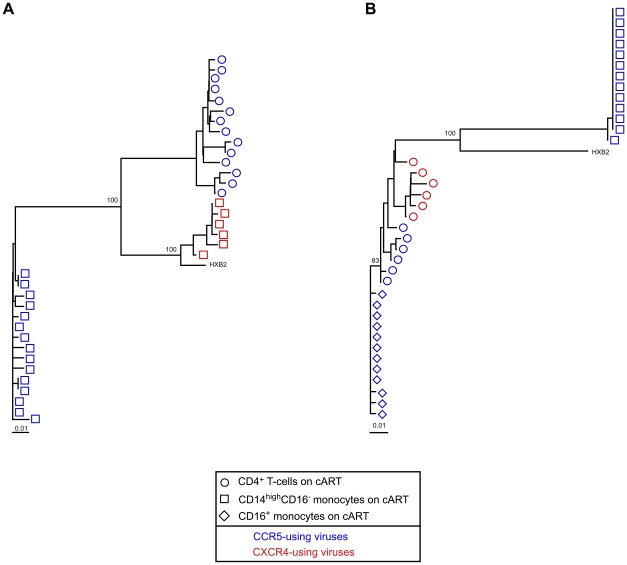
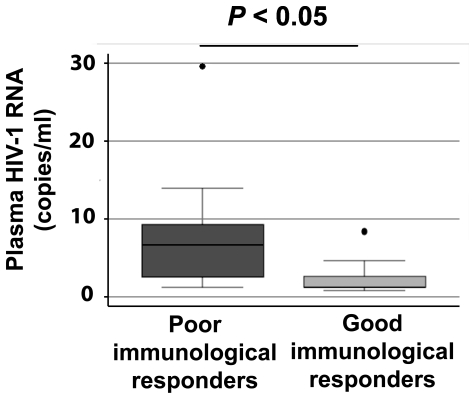
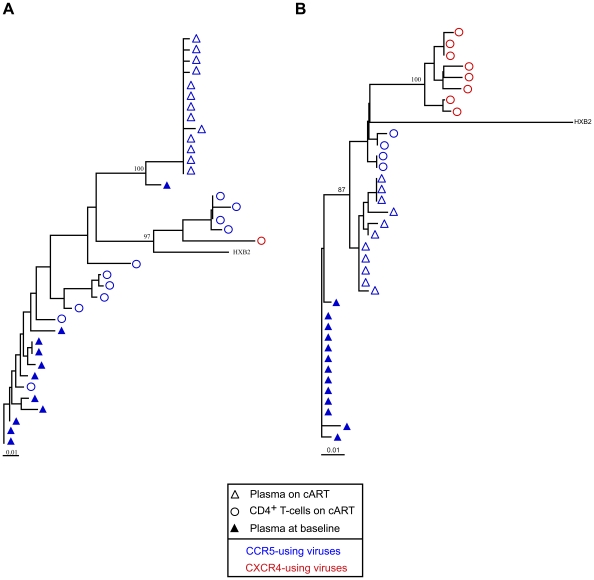
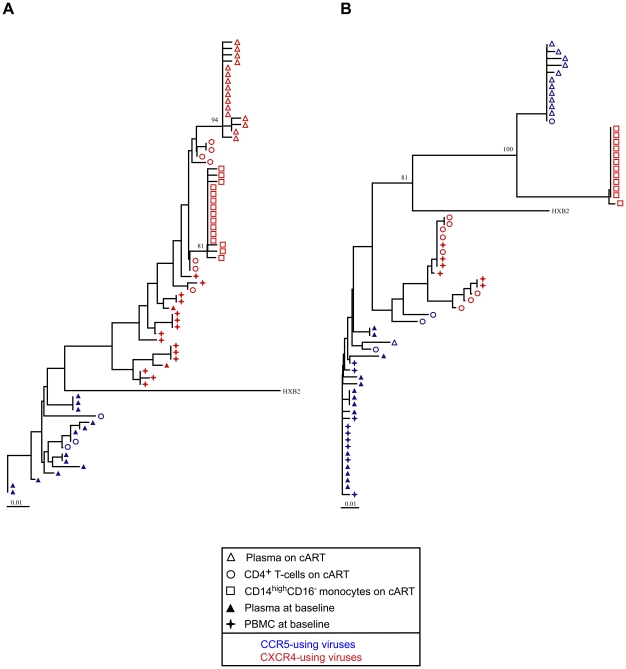
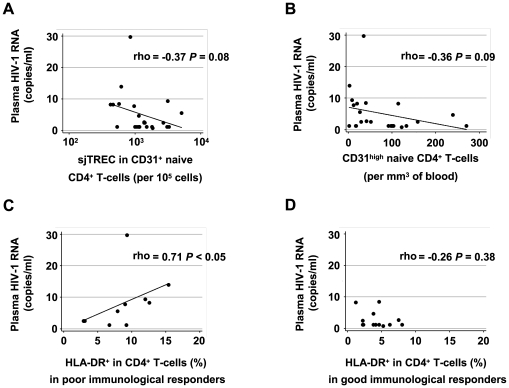
Methodology/principal findings: We characterized the recently produced residual viruses in the plasma and short-lived blood monocytes of 23 patients with various immunological responses to sustained suppressive cART. We quantified the residual HIV-1 in the plasma below 50 copies/ml, and in the CD14(high) CD16(-) and CD16+ monocyte subsets sorted by flow cytometry, and predicted coreceptor usage by genotyping V3 env sequences. We detected residual viremia in the plasma of 8 of 10 patients with poor CD4+ T-cell reconstitution in response to cART and in only 5 of 13 patients with good CD4+ T-cell reconstitution. CXCR4-using viruses were frequent among the recently produced viruses in the plasma and in the main CD14(high) CD16(-) monocyte subset. Finally, the residual viremia was correlated with persistent CD4+ and CD8+ T-cell activation in patients with poor immune reconstitution.
Conclusions: Low-level viremia could result from the release of archived viruses from cellular reservoirs and/or from ongoing virus replication in some patients. The compartmentalization of the viruses between the plasma and the blood monocytes suggests at least two origins of residual virus production during effective cART. CXCR4-using viruses might be produced preferentially in patients on cART. Our results also suggest that low-level HIV-1 production in some patients may contribute to persistent immune dysfunction despite cART.
Conflict of interest statement
Figures
Similar articles
-
Anti-Tat immunity defines CD4+ T-cell dynamics in people living with HIV on long-term cART.EBioMedicine. 2021 Apr;66:103306. doi: 10.1016/j.ebiom.2021.103306. Epub 2021 Apr 7. EBioMedicine. 2021. PMID: 33839064 Free PMC article.
-
Naive T-cell depletion related to infection by X4 human immunodeficiency virus type 1 in poor immunological responders to highly active antiretroviral therapy.J Virol. 2006 Oct;80(20):10229-36. doi: 10.1128/JVI.00965-06. J Virol. 2006. PMID: 17005700 Free PMC article.
-
Evidence for human immunodeficiency virus type 1 replication in vivo in CD14(+) monocytes and its potential role as a source of virus in patients on highly active antiretroviral therapy.J Virol. 2002 Jan;76(2):707-16. doi: 10.1128/jvi.76.2.707-716.2002. J Virol. 2002. PMID: 11752161 Free PMC article.
-
Potential implication of residual viremia in patients on effective antiretroviral therapy.AIDS Res Hum Retroviruses. 2015 Jan;31(1):25-35. doi: 10.1089/AID.2014.0194. AIDS Res Hum Retroviruses. 2015. PMID: 25428885 Free PMC article. Review.
-
Can HIV infection be eradicated through use of potent antiviral agents?Curr Opin Infect Dis. 2010 Dec;23(6):628-32. doi: 10.1097/QCO.0b013e32833ff1d0. Curr Opin Infect Dis. 2010. PMID: 20847693 Review.
Cited by
-
Interleukin 10 responses are associated with sustained CD4 T-cell counts in treated HIV infection.J Infect Dis. 2012 Sep 1;206(5):780-9. doi: 10.1093/infdis/jis380. Epub 2012 Jun 12. J Infect Dis. 2012. PMID: 22693231 Free PMC article.
-
Discordance between peripheral and colonic markers of inflammation during suppressive ART.J Acquir Immune Defic Syndr. 2014 Feb 1;65(2):133-41. doi: 10.1097/01.qai.0000437172.08127.0b. J Acquir Immune Defic Syndr. 2014. PMID: 24121758 Free PMC article.
-
HIV induces production of IL-18 from intestinal epithelial cells that increases intestinal permeability and microbial translocation.PLoS One. 2018 Mar 30;13(3):e0194185. doi: 10.1371/journal.pone.0194185. eCollection 2018. PLoS One. 2018. PMID: 29601578 Free PMC article.
-
Serious Non-AIDS events: Immunopathogenesis and interventional strategies.AIDS Res Ther. 2013 Dec 13;10(1):29. doi: 10.1186/1742-6405-10-29. AIDS Res Ther. 2013. PMID: 24330529 Free PMC article.
-
Time course of cellular HIV-DNA and low-level HIV viremia in HIV-HCV co-infected patients whose HCV infection had been successfully treated with directly acting antivirals.Med Microbiol Immunol. 2017 Dec;206(6):419-428. doi: 10.1007/s00430-017-0518-x. Epub 2017 Sep 1. Med Microbiol Immunol. 2017. PMID: 28864951
References
-
- Dornadula G, Zhang H, VanUitert B, Stern J, Livornese L, Jr, et al. Residual HIV-1 RNA in blood plasma of patients taking suppressive highly active antiretroviral therapy. Jama. 1999;282:1627–1632. - PubMed
-
- Havlir DV, Strain MC, Clerici M, Ignacio C, Trabattoni D, et al. Productive infection maintains a dynamic steady state of residual viremia in human immunodeficiency virus type 1-infected persons treated with suppressive antiretroviral therapy for five years. J Virol. 2003;77:11212–11219. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
