

Cryotherapy for breast cancer: a feasibility study without excision
- PMID: 19800542
- PMCID: PMC3865783
- DOI: 10.1016/j.jvir.2009.06.029
Cryotherapy for breast cancer: a feasibility study without excision
Abstract
Purpose: To assess the feasibility of percutaneous multiprobe breast cryoablation (BC) for diverse presentations of cancers that remained in situ after BC.
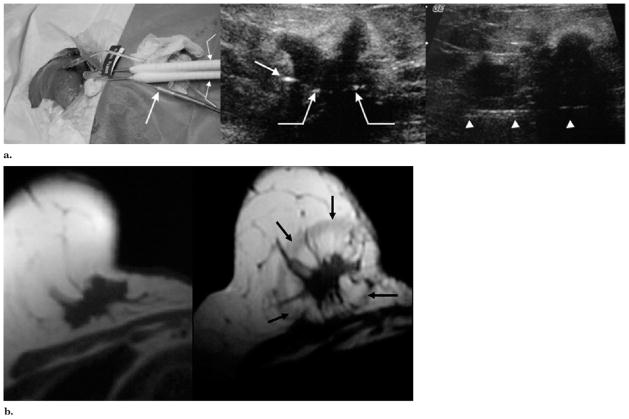
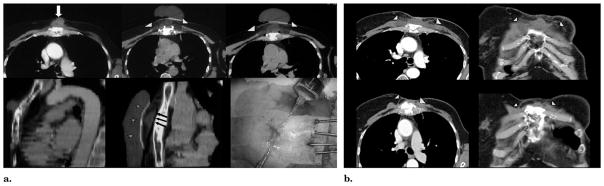
Materials and methods: After breast magnetic resonance (MR) imaging and thorough consultation, patients underwent BC after giving informed consent. This study was approved by the institutional review board. In 12 BC sessions, 22 breast cancer foci (stages I-IV) were treated in 11 patients who refused surgery by using multiple 2.4-mm cryoprobes. Five patients had recurrent disease and six had new diagnoses. With use of only local anesthesia, six patients were treated with ultrasonographic (US) guidance and five were treated with both computed tomographic (CT) and US guidance. Saline injections and warming bags were used to protect the skin. Procedure success was defined as 1 cm visible ice beyond all tumor margins. MR imaging and/or clinical follow-up were available for up to 72 months after BC.
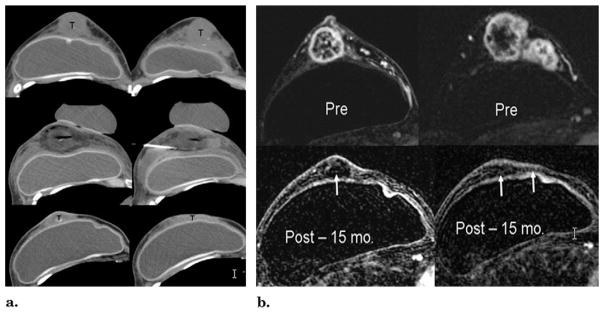
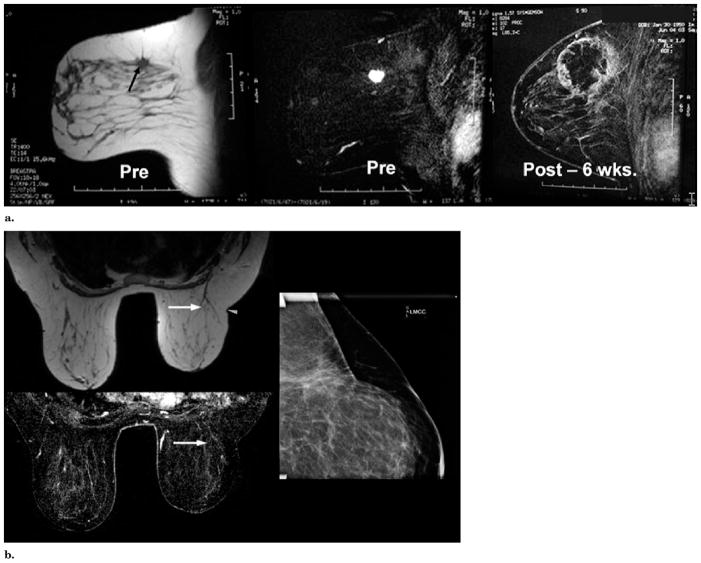
Results: US produced sufficient ice visualization for small tumors, whereas CT helped confirm overall ice extent. The mean pretreatment breast tumor diameter was 1.7 cm +/- 1.2 (range, 0.5-5.8 cm), and an average of 3.1 cryoprobes produced 100% procedural success with mean ice diameters of 5.1 cm +/- 2.2 (range, 2.0-10.0 cm). No significant complications, retraction, or scarring were noted. Biopsies at the margins of the cryoablation site immediately after BC and at follow-up were all negative. No local recurrences have been noted at an average imaging follow-up of 18 months.
Conclusions: In conjunction with thorough pre- and postablation MR imaging, CT/US-guided multiprobe BC safely achieved 1 cm visible ice beyond tumor margins with minimal discomfort, good cosmesis, and no short-term local tumor recurrences.
Conflict of interest statement
None of the other authors have identified a conflict of interest.
Figures

Similar articles
-
Small (< 2.0-cm) breast cancers: mammographic and US findings at US-guided cryoablation--initial experience.Radiology. 2004 Dec;233(3):857-67. doi: 10.1148/radiol.2333031734. Radiology. 2004. PMID: 15567802 Clinical Trial.
-
Real-time magnetic resonance imaging-guided cryoablation of small renal tumors at 1.5 T.Invest Radiol. 2013 Jun;48(6):437-44. doi: 10.1097/RLI.0b013e31828027c2. Invest Radiol. 2013. PMID: 23511191 Free PMC article. Clinical Trial.
-
Cryotherapy for breast fibroadenomas.Radiology. 2005 Jan;234(1):63-72. doi: 10.1148/radiol.2341030931. Epub 2004 Nov 18. Radiology. 2005. PMID: 15550369 Clinical Trial.
-
Percutaneous cryoablation of hepatic tumors: long-term experience of a large U.S. series.Abdom Radiol (NY). 2016 Apr;41(4):767-80. doi: 10.1007/s00261-016-0687-x. Abdom Radiol (NY). 2016. PMID: 26960728 Review.
-
Percutaneous Image-Guided Cryoablation of Breast Cancer: A Systematic Review.J Vasc Interv Radiol. 2015 Nov;26(11):1652-7.e1. doi: 10.1016/j.jvir.2015.07.020. Epub 2015 Sep 3. J Vasc Interv Radiol. 2015. PMID: 26342882 Review.
Cited by
-
CT-Guided Percutaneous Cryoablation of Breast Cancer: A Single-Center Experience.Cancers (Basel). 2024 Jun 28;16(13):2373. doi: 10.3390/cancers16132373. Cancers (Basel). 2024. PMID: 39001435 Free PMC article.
-
Image-guided tumor ablation: emerging technologies and future directions.Semin Intervent Radiol. 2010 Sep;27(3):302-13. doi: 10.1055/s-0030-1261789. Semin Intervent Radiol. 2010. PMID: 22550370 Free PMC article.
-
Percutaneous Cryoablation of Metastatic Lesions from Colorectal Cancer: Efficacy and Feasibility with Survival and Cost-Effectiveness Observations.ISRN Minim Invasive Surg. 2012;2012:942364. doi: 10.5402/2012/942364. ISRN Minim Invasive Surg. 2012. PMID: 25621178 Free PMC article.
-
Cryosurgery for primary breast cancers, its biological impact, and clinical outcomes.Int J Clin Oncol. 2019 Jun;24(6):608-613. doi: 10.1007/s10147-019-01448-4. Epub 2019 Apr 13. Int J Clin Oncol. 2019. PMID: 30982153 Review.
-
Breast cancer cryoablation with radiologic-pathologic correlation.Br J Radiol. 2022 Dec 1;95(1140):20220480. doi: 10.1259/bjr.20220480. Epub 2022 Sep 5. Br J Radiol. 2022. PMID: 36000723 Free PMC article. Review.
References
-
- van Esser S, van den Bosch MA, van Diest PJ, Mali WT, Borel Rinkes IH, van Hillegersberg R. Minimally invasive ablative therapies for invasive breast carcinomas: an overview of current literature. World J Surg. 2007;31:2284–2292. - PubMed
-
- Huston TL, Simmons RM. Ablative therapies for the treatment of malignant diseases of the breast. Am J Surg. 2005;189:694–701. - PubMed
-
- Rubinsky B. Irreversible electroporation in medicine. Technol Cancer Res Treat. 2007;6:255–260. - PubMed
-
- Kaiser WA, Pfleiderer SO, Baltzer PA. MRI-guided interventions of the breast. J Magn Reson Imaging. 2008;27:347–355. - PubMed
-
- Lehman CD, Isaacs C, Schnall MD, et al. Cancer yield of mammography, MR, and US in high-risk women: prospective multi-institution breast cancer screening study. Radiology. 2007;244:381–388. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
