

Cytotoxic T lymphocyte therapy with donor T cells prevents and treats adenovirus and Epstein-Barr virus infections after haploidentical and matched unrelated stem cell transplantation
- PMID: 19700662
- PMCID: PMC2774556
- DOI: 10.1182/blood-2009-07-232454
Cytotoxic T lymphocyte therapy with donor T cells prevents and treats adenovirus and Epstein-Barr virus infections after haploidentical and matched unrelated stem cell transplantation
Abstract
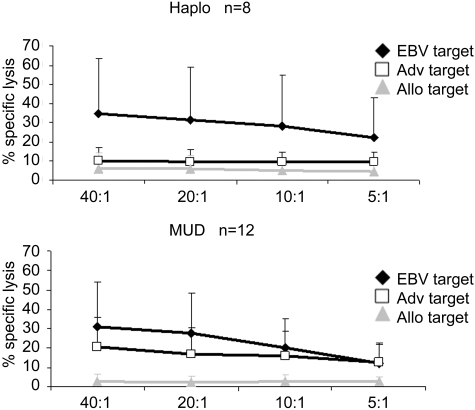
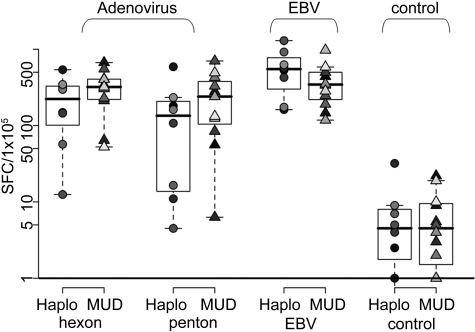
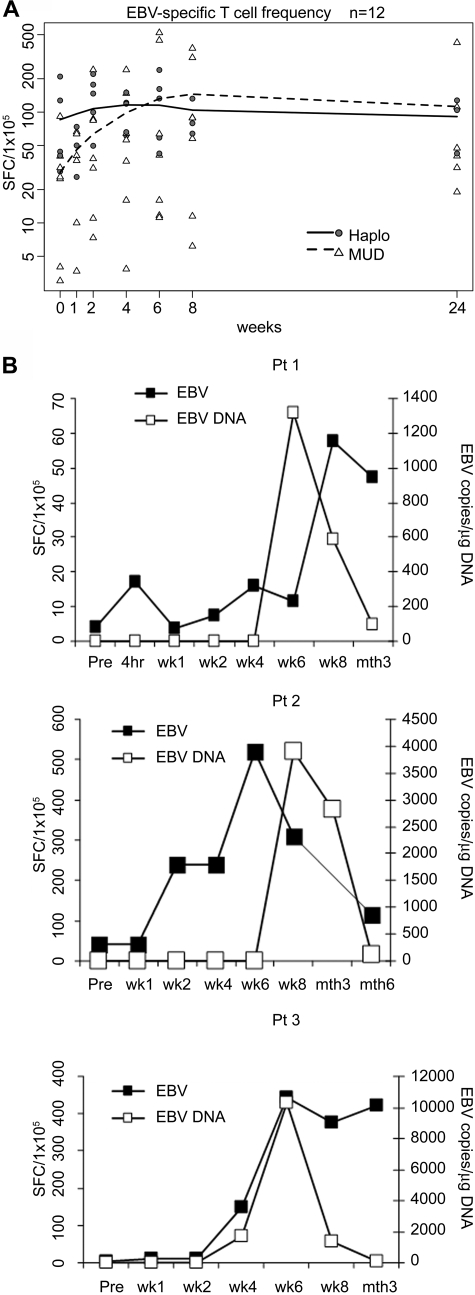
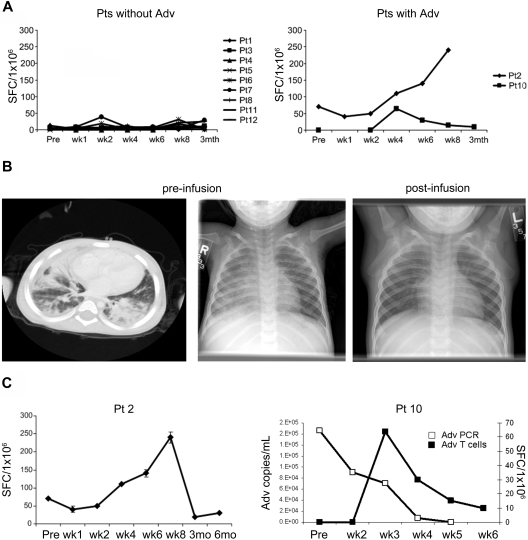
Viral infection or reactivation remains a major cause of morbidity and mortality after allogeneic stem cell transplantation. We now show that infusions of single cytotoxic T lymphocyte (CTL) lines (5 x 10(6)-1.35 x 10(8) cells/m(2)) with specificity for 2 commonly detected viruses, Epstein-Barr virus (EBV) and adenovirus, can be safely administered to pediatric transplantation recipients receiving partially human leukocyte antigen-matched and haploidentical stem cell grafts (n = 13), without inducing graft-versus-host disease. The EBV-specific component of the CTLs expanded in vivo and persisted for more than 12 weeks, but the adenovirus-specific component only expanded in vivo in the presence of concomitant adenoviral infection. Nevertheless, adenovirus-specific T cells could be detected for at least 8 weeks in peripheral blood, even in CTL recipients without viral infection, provided the adenovirus-specific component of their circulating lymphocytes was first expanded by exposure to adenoviral antigens ex vivo. After infusion, none of these 13 high-risk recipients developed EBV-associated lymphoproliferative disease, while 2 of the subjects had resolution of their adenoviral disease. Hence, bispecific CTLs containing both EBV- and adenovirus-specific T cells can safely reconstitute an antigen responsive "memory" population of CTLs after human leukocyte antigen-mismatched stem cell transplantation and may provide antiviral activity. This trial was registered at www.clinicaltrials.gov as #NCT00590083.
Figures


Similar articles
-
Epstein-Barr virus (EBV) load in bone marrow transplant recipients at risk to develop posttransplant lymphoproliferative disease: prophylactic infusion of EBV-specific cytotoxic T cells.Blood. 2000 Feb 1;95(3):807-14. Blood. 2000. PMID: 10648390
-
An Epstein-Barr virus deletion mutant associated with fatal lymphoproliferative disease unresponsive to therapy with virus-specific CTLs.Blood. 2001 Feb 15;97(4):835-43. doi: 10.1182/blood.v97.4.835. Blood. 2001. PMID: 11159505
-
Curative or pre-emptive adenovirus-specific T cell transfer from matched unrelated or third party haploidentical donors after HSCT, including UCB transplantations: a successful phase I/II multicenter clinical trial.J Hematol Oncol. 2017 May 8;10(1):102. doi: 10.1186/s13045-017-0469-0. J Hematol Oncol. 2017. PMID: 28482908 Free PMC article. Clinical Trial.
-
Strategies of adoptive T -cell transfer to treat refractory viral infections post allogeneic stem cell transplantation.J Hematol Oncol. 2019 Feb 6;12(1):13. doi: 10.1186/s13045-019-0701-1. J Hematol Oncol. 2019. PMID: 30728058 Free PMC article. Review.
-
Epstein-Barr virus-specific cytotoxic T-lymphocytes for adoptive immunotherapy of post-transplant lymphoproliferative disease.Blood Rev. 2004 Sep;18(3):193-209. doi: 10.1016/j.blre.2003.12.002. Blood Rev. 2004. PMID: 15183903 Review.
Cited by
-
Short-term in-vitro expansion improves monitoring and allows affordable generation of virus-specific T-cells against several viruses for a broad clinical application.PLoS One. 2013 Apr 22;8(4):e59592. doi: 10.1371/journal.pone.0059592. Print 2013. PLoS One. 2013. PMID: 23630567 Free PMC article.
-
CMVpp65 Vaccine Enhances the Antitumor Efficacy of Adoptively Transferred CD19-Redirected CMV-Specific T Cells.Clin Cancer Res. 2015 Jul 1;21(13):2993-3002. doi: 10.1158/1078-0432.CCR-14-2920. Epub 2015 Apr 2. Clin Cancer Res. 2015. PMID: 25838392 Free PMC article.
-
Human papillomavirus type 16 E6/E7-specific cytotoxic T lymphocytes for adoptive immunotherapy of HPV-associated malignancies.J Immunother. 2013 Jan;36(1):66-76. doi: 10.1097/CJI.0b013e318279652e. J Immunother. 2013. PMID: 23211628 Free PMC article.
-
Preventing stem cell transplantation-associated viral infections using T-cell therapy.Immunotherapy. 2015;7(7):793-810. doi: 10.2217/imt.15.43. Epub 2015 Aug 7. Immunotherapy. 2015. PMID: 26250410 Free PMC article. Review.
-
NK Cell Reconstitution in Paediatric Leukemic Patients after T-Cell-Depleted HLA-Haploidentical Haematopoietic Stem Cell Transplantation Followed by the Reinfusion of iCasp9-Modified Donor T Cells.J Clin Med. 2019 Nov 7;8(11):1904. doi: 10.3390/jcm8111904. J Clin Med. 2019. PMID: 31703320 Free PMC article.
References
-
- Chakrabarti S, Mautner V, Osman H, et al. Adenovirus infections following allogeneic stem cell transplantation: incidence and outcome in relation to graft manipulation, immunosuppression, and immune recovery. Blood. 2002;100(5):1619–1627. - PubMed
-
- Chakrabarti S, MacKinnon S, Chopra R, et al. High incidence of cytomegalovirus infection after nonmyeloablative stem cell transplantation: potential role of Campath-1H in delaying immune reconstitution. Blood. 2002;99(12):4357–4363. - PubMed
-
- Heslop HE, Ng CYC, Li C, et al. Long-term restoration of immunity against Epstein-Barr virus infection by adoptive transfer of gene-modified virus-specific T lymphocytes. Nat Med. 1996;2:551–555. - PubMed
-
- Walter EA, Greenberg PD, Gilbert MJ, et al. Reconstitution of cellular immunity against cytomegalovirus in recipients of allogeneic bone marrow by transfer of T-cell clones from the donor. N Engl J Med. 1995;333(16):1038–1044. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
