Use of 18F-fluorodeoxyglucose positron emission tomography in patients with rare head and neck cancers
- PMID: 19434281
- PMCID: PMC2671791
- DOI: 10.3342/ceo.2008.1.2.103
Use of 18F-fluorodeoxyglucose positron emission tomography in patients with rare head and neck cancers
Abstract
Objectives: The clinical utility of (18)F-fluorodeoxyglucose (FDG) positron emission tomography (PET) has been demonstrated in major head and neck cancers (HNCs) but is unclear in rare HNCs. We therefore evaluated FDG PET in the management of patients with rare HNCs.
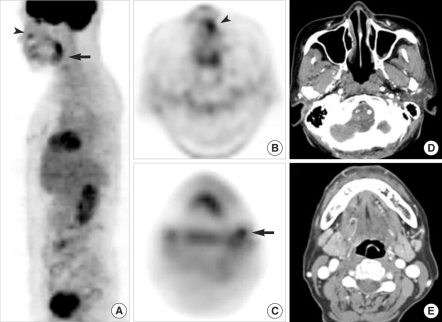
Methods: FDG PET and CT/MRI scanning were performed at the initial staging and/or the follow-up in 24 patients with rare HNCs, 10 with melanoma, 9 with sarcoma, 3 with olfactory neuroblastomas, and 2 with basal cell carcinoma. The diagnostic accuracy of CT and FDG PET for detecting primary tumors and metastases were compared with a histopathologic reference. The association between the PET results and the clinicopathologic parameters predicting tumor invasion, histologic grade and disease-free survival (DFS), was assessed.
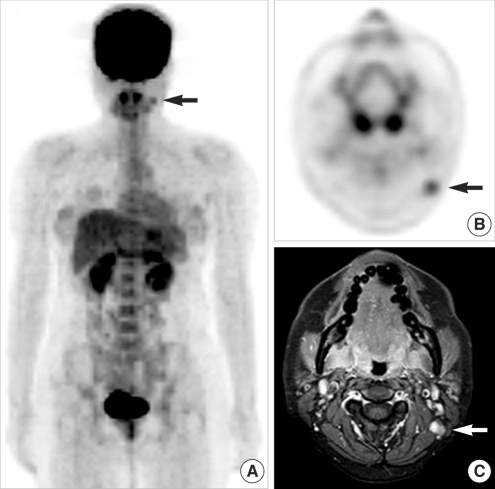
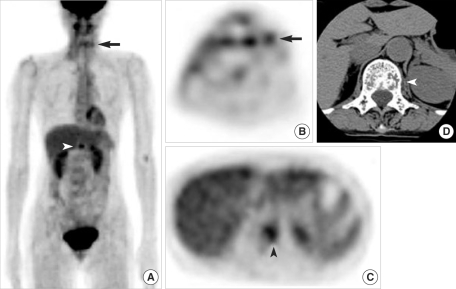
Results: The overall accuracies of FDG PET and CT/MRI were 92% and 79%, respectively, for detecting primary tumors and 91% and 74%, respectively, for nodal metastases, but the differences were not significant due to the small number of patients. The sensitivity and specificity of FDG PET for detecting distant metastases and second primary tumors were 100% and 87%, respectively. Follow-up FDG PET correctly diagnosed locoregional recurrence in all 12 patients, as shown by biopsy, and distant metastases in 6 patients. However, thickness of melanoma, histologic grade of sarcoma, and DFS were not associated with tumor FDG uptake.
Conclusion: FDG PET may be useful for staging, posttreatment monitoring, and detection of distant metastases and second primary tumors in patients with rare HNCs.
Keywords: Fluorodeoxyglucose; Head and neck neoplasms; Neoplasm staging; Positron-emission tomography; Surveillance.
Figures
Similar articles
-
Clinical utility of 18F-FDG PET for patients with salivary gland malignancies.J Nucl Med. 2007 Feb;48(2):240-6. J Nucl Med. 2007. PMID: 17268021
-
Combined 18F-fluorodeoxyglucose-positron emission tomography and computed tomography as a primary screening method for detecting second primary cancers and distant metastases in patients with head and neck cancer.Ann Oncol. 2007 Oct;18(10):1698-703. doi: 10.1093/annonc/mdm270. Epub 2007 Aug 22. Ann Oncol. 2007. PMID: 17716985
-
Utility of combined (18)F-fluorodeoxyglucose-positron emission tomography and computed tomography in patients with cervical metastases from unknown primary tumors.Oral Oncol. 2009 Mar;45(3):218-24. doi: 10.1016/j.oraloncology.2008.05.010. Epub 2008 Sep 18. Oral Oncol. 2009. PMID: 18804404
-
Overview of the clinical effectiveness of positron emission tomography imaging in selected cancers.Health Technol Assess. 2007 Oct;11(44):iii-iv, xi-267. doi: 10.3310/hta11440. Health Technol Assess. 2007. PMID: 17999839 Review.
-
The diagnostic accuracy of 18F-fluorodeoxyglucose positron emission tomography and computed tomography in staging bladder cancer: a single-institution study and a systematic review with meta-analysis.World J Urol. 2016 Sep;34(9):1229-37. doi: 10.1007/s00345-016-1772-z. Epub 2016 Feb 4. World J Urol. 2016. PMID: 26847182 Review.
Cited by
-
Diagnostic Performance of [18F]F-FDG Positron Emission Tomography (PET) in Non-Ophthalmic Malignant Melanoma: A Systematic Review and Meta-Analysis of More Than 10,000 Melanoma Patients.Cancers (Basel). 2024 Jan 2;16(1):215. doi: 10.3390/cancers16010215. Cancers (Basel). 2024. PMID: 38201642 Free PMC article. Review.
-
123I-MIBG scintigraphy and 18F-FDG-PET imaging for diagnosing neuroblastoma.Cochrane Database Syst Rev. 2015 Sep 29;2015(9):CD009263. doi: 10.1002/14651858.CD009263.pub2. Cochrane Database Syst Rev. 2015. PMID: 26417712 Free PMC article. Review.
-
Pretreatment tumor SUVmax predicts disease-specific and overall survival in patients with head and neck soft tissue sarcoma.Eur J Nucl Med Mol Imaging. 2017 Jan;44(1):33-40. doi: 10.1007/s00259-016-3456-8. Epub 2016 Jul 23. Eur J Nucl Med Mol Imaging. 2017. PMID: 27448574
-
Ultrasound, CT, MRI, or PET-CT for staging and re-staging of adults with cutaneous melanoma.Cochrane Database Syst Rev. 2019 Jul 1;7(7):CD012806. doi: 10.1002/14651858.CD012806.pub2. Cochrane Database Syst Rev. 2019. PMID: 31260100 Free PMC article.
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007 Jan–Feb;57(1):43–66. - PubMed
-
- Zimmer LA, Branstetter BF, Nayak JV, Johnson JT. Current use of 18F-fluorodeoxyglucose positron emission tomography and combined positron emission tomography and computed tomography in squamous cell carcinoma of the head and neck. Laryngoscope. 2005 Nov;115(11):2029–2034. - PubMed
-
- Menda Y, Graham MM. Update on 18F-fluorodeoxyglucose/positron emission tomography and positron emission tomography/computed tomography imaging of squamous head and neck cancers. Semin Nucl Med. 2005 Oct;35(4):214–219. - PubMed
-
- Kostakoglu L, Leonard JP, Kuji I, Coleman M, Vallabhajosula S, Goldsmith SJ. Comparison of fluorine-18 fluorodeoxyglucose positron emission tomography and Ga-67 scintigraphy in evaluation of lymphoma. Cancer. 2002 Feb 15;94(4):879–888. - PubMed
-
- Schöder H, Yeung HW. Positron emission imaging of head and neck cancer, including thyroid carcinoma. Semin Nucl Med. 2004 Jul;34(3):180–197. - PubMed