

Review
doi: 10.1007/s00125-009-1321-z.
Epub 2009 Mar 27.
The beta cell lesion in type 2 diabetes: there has to be a primary functional abnormality
Affiliations
- PMID: 19326096
- PMCID: PMC2737455
- DOI: 10.1007/s00125-009-1321-z
Item in Clipboard
Review
The beta cell lesion in type 2 diabetes: there has to be a primary functional abnormality
Diabetologia.
2009 Jun.
Abstract
The critical role of the beta cell in the pathogenesis of type 2 diabetes is now well established. When examined in patients with type 2 diabetes and individuals at increased risk, reductions in beta cell mass and abnormalities of beta cell function can both be demonstrated. The question of whether one alone is sufficient or both are necessary for the development of hyperglycaemia has been debated. Based on human and animal studies, it appears that neither alone is sufficient. Rather, for glucose to rise to the level at which diabetes would be diagnosed, defects in beta cell mass and in beta cell function are required.
Conflict of interest statement
The authors declare that they have no duality of interest.
Figures
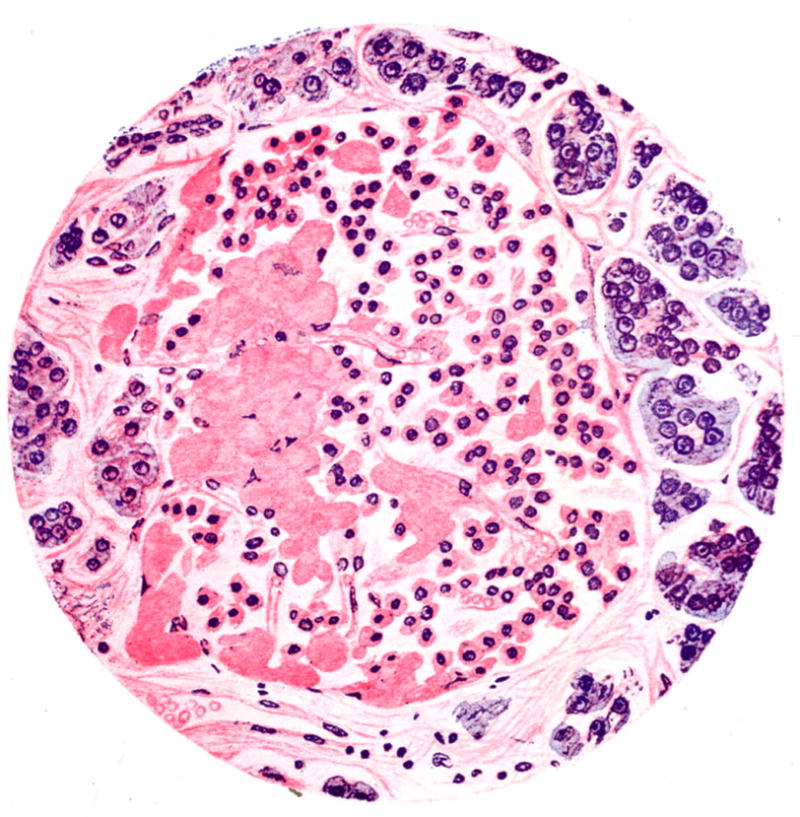
Hand drawn micrograph of an islet from a patient with type 2 diabetes stained with haematoxylin and eosin. Cellularity of the islet is decreased and it contains eosinophilic material termed “hyalinosis”, which we now know as amyloid. Reprinted with permission from [3].
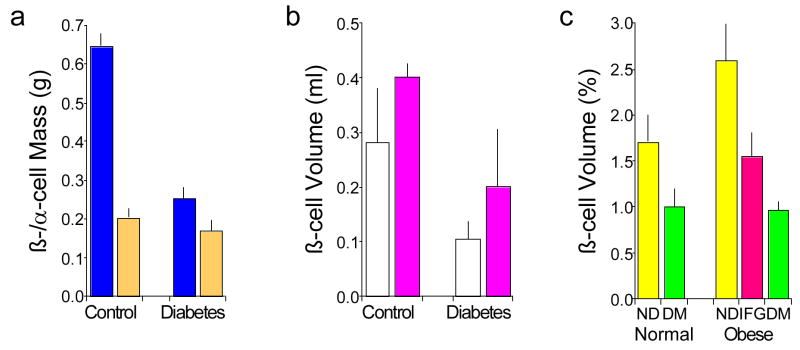
Relationship of obesity and glucose tolerance with islet beta and alpha cell volume and mass based on autopsy assessments. (a) Beta cell mass (blue) is reduced in subjects with type 2 diabetes (n=25) compared to controls (n=25), while alpha cell mass (orange) is not different. Subjects with type 1 diabetes and those with amyloidosis were excluded. Data are mean ± se and from [4] with permission. (b) Beta cell volume is increased in obese (pink; n=4 controls and 6 with type 2 diabetes) compared to normal weight (white; n=7 controls and 8 with type 2 diabetes) subjects. Diabetes is associated with reduced beta cell volume in both obese and normal weight subjects. Data are mean ± sd and from [5] with permission. (c) Beta cell volume is reduced in subjects with type 2 diabetes (DM, green; n=16 normal weight and 41 obese) compared to those who do not have diabetes (ND, yellow; n=17 normal weight and 31 obese), whether subjects are normal weight of obese. Subjects with impaired fasting glucose (IFG, pink; n=19 obese) have reduced beta cell volume that is intermediate between no diabetes and diabetes. Data are mean ± se and adapted with permission from [6].
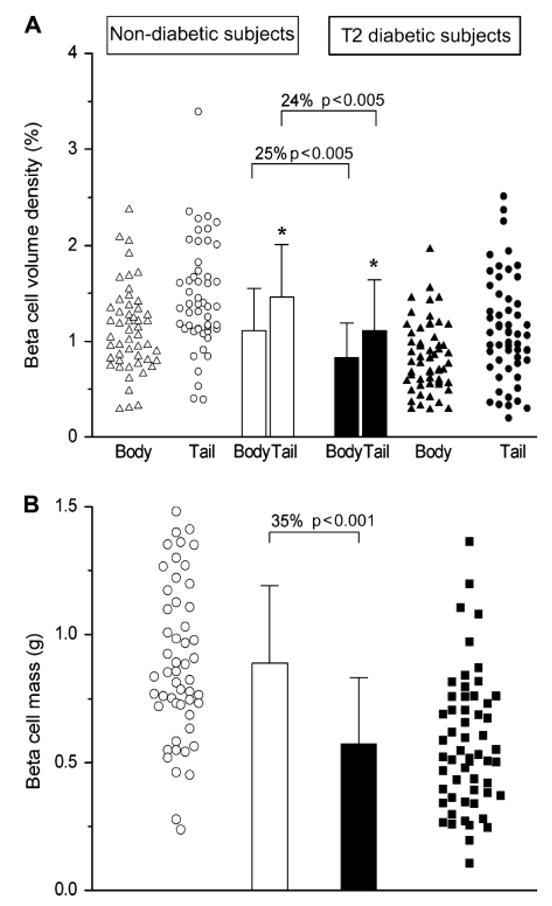
Differences in beta cell volume and mass in 52 subjects without (open symbols and bars) and 57 with type 2 diabetes (closed symbols and bars). (a) The volume of beta cells varies markedly in non-diabetic and diabetic subjects with a lot of overlap between the two groups. Despite this large variability, beta cell volume is greater in the pancreatic tail than body in both non-diabetic and diabetic subjects. In subjects with diabetes compared to those without, beta cell volume is reduced in both the body and tail of the pancreas. (b) Beta cell mass determined based on volume density and pancreatic weight is reduced by 35% in subjects with type 2 diabetes. Data are mean ± sd. Reproduced with permission from [12].
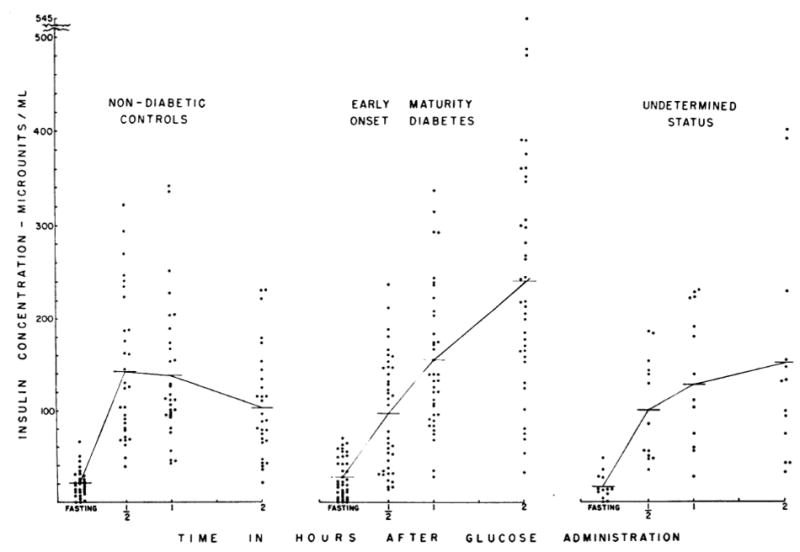
Plasma insulin concentrations before and following a 100-gram glucose load in healthy control subjects and two groups of subjects, one known to have early (“maturity onset”) type 2 diabetes and a second group in whom the duration of the diabetes was undetermined. The insulin response at 30 minutes was clearly diminished in individuals with recent onset of hyperglycaemia. Reproduced with permission from [26].
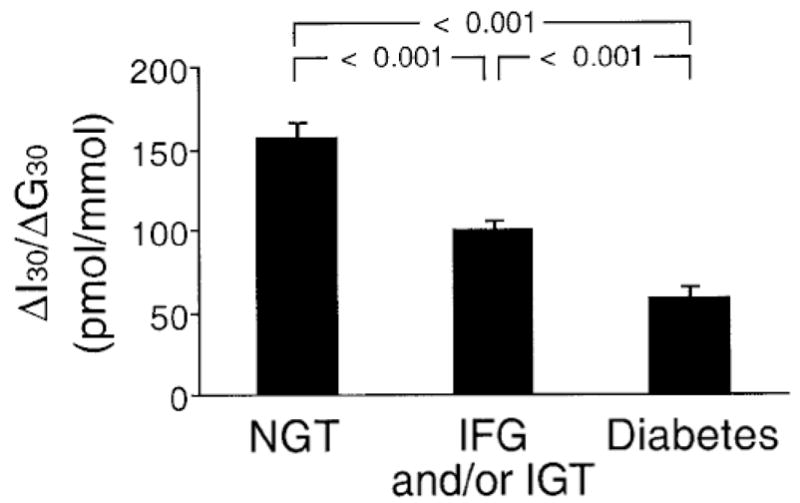
Incremental early insulin response (insulinogenic index) measured 30 minutes after glucose ingestion (ΔI30/ΔG30) in 240 subjects with normal glucose tolerance (NGT), 191 with impaired fasting glucose/impaired glucose tolerance (IFG/IGT) and 100 with diabetes. As glucose tolerance declined, beta cell function deteriorated. Reproduced with permission from [27].
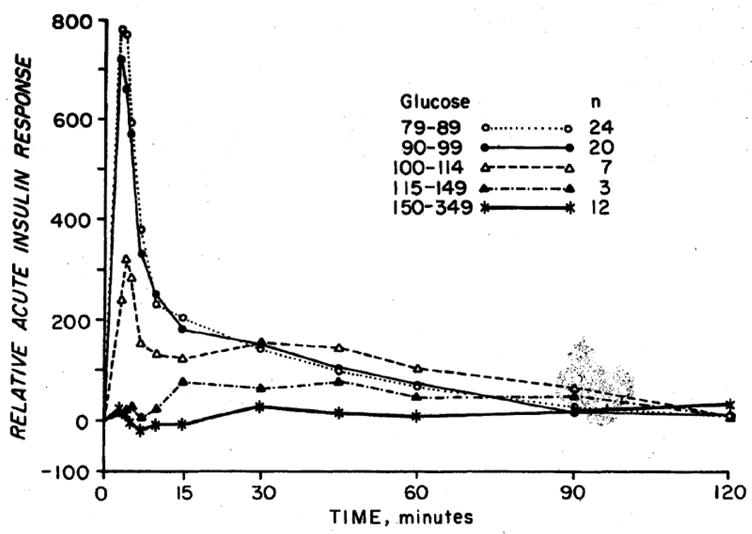
Acute insulin response to intravenous glucose in subjects grouped based on their fasting glucose levels. As the fasting glucose increases, the insulin response decreases. The response is absent when fasting glucose exceeds 6.4 mmol/l. Reproduced with permission from [30].
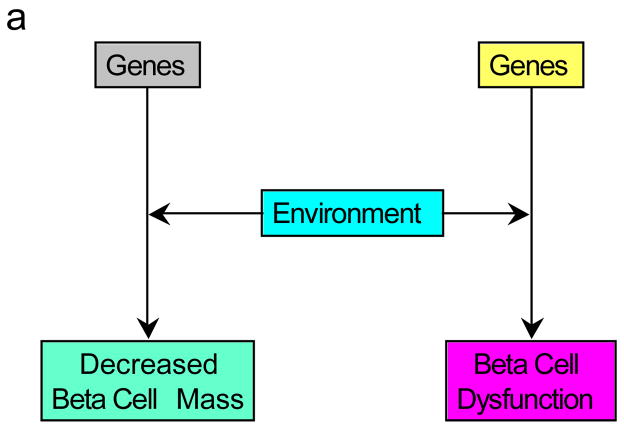
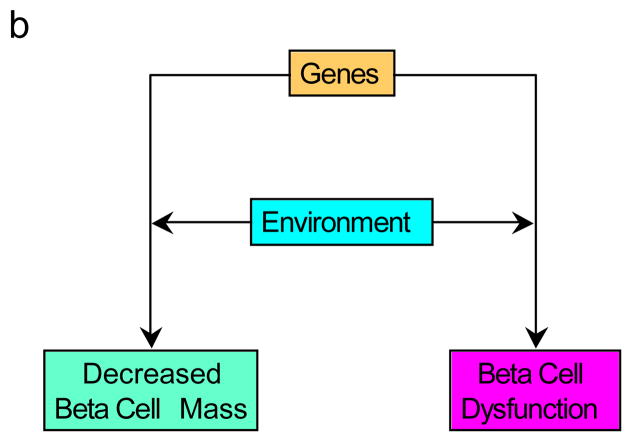
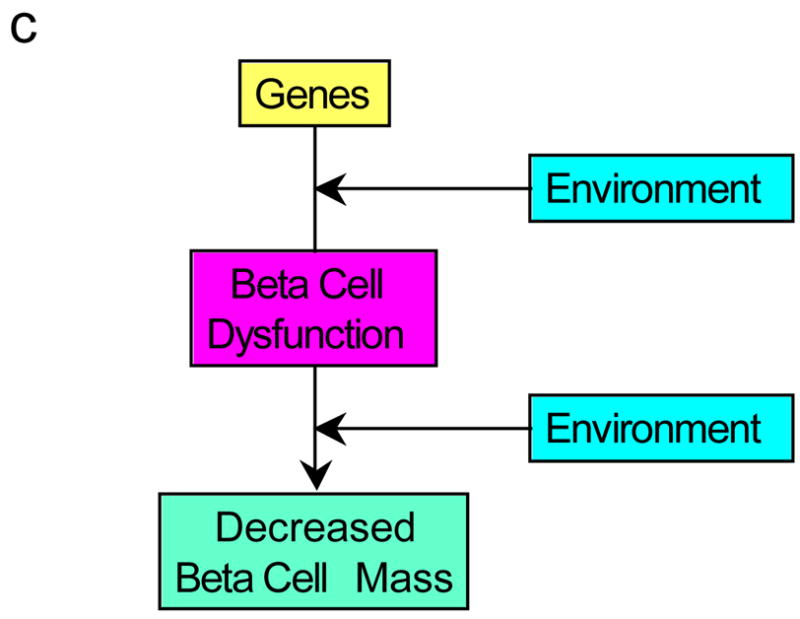
Possible pathways for the development of the reduced beta cell mass and beta cell dysfunction observed in type 2 diabetes. (a) Genetic defects combined with environmental changes determine reductions in both beta cell function and mass. (b) A genetic defect in combination with environmental changes simultaneously affects both mass and function. (c) The interaction of genetic susceptibility with environmental factors results in beta cell dysfunction that in turn leads to a loss of beta cells. The effect of this combination of changes is associated with the development of hyperglycaemia.
Possible pathways for the development of the reduced beta cell mass and beta cell dysfunction observed in type 2 diabetes. (a) Genetic defects combined with environmental changes determine reductions in both beta cell function and mass. (b) A genetic defect in combination with environmental changes simultaneously affects both mass and function. (c) The interaction of genetic susceptibility with environmental factors results in beta cell dysfunction that in turn leads to a loss of beta cells. The effect of this combination of changes is associated with the development of hyperglycaemia.
Possible pathways for the development of the reduced beta cell mass and beta cell dysfunction observed in type 2 diabetes. (a) Genetic defects combined with environmental changes determine reductions in both beta cell function and mass. (b) A genetic defect in combination with environmental changes simultaneously affects both mass and function. (c) The interaction of genetic susceptibility with environmental factors results in beta cell dysfunction that in turn leads to a loss of beta cells. The effect of this combination of changes is associated with the development of hyperglycaemia.
Similar articles
-
Role of reduced β-cell mass versus impaired β-cell function in the pathogenesis of type 2 diabetes.Diabetes Care. 2013 Aug;36 Suppl 2(Suppl 2):S113-9. doi: 10.2337/dcS13-2008. Diabetes Care. 2013. PMID: 23882035 Free PMC article. No abstract available.
-
Assessment of β-cell function in human patients.Islets. 2012 Mar-Apr;4(2):79-83. doi: 10.4161/isl.19270. Epub 2012 Mar 1. Islets. 2012. PMID: 22627463 Review.
-
Dysfunction of Persisting β Cells Is a Key Feature of Early Type 2 Diabetes Pathogenesis.Cell Rep. 2020 Apr 7;31(1):107469. doi: 10.1016/j.celrep.2020.03.033. Cell Rep. 2020. PMID: 32268101
-
Beta-cell function and mass in type 2 diabetes.Dan Med Bull. 2009 Aug;56(3):153-64. Dan Med Bull. 2009. PMID: 19728971
-
Beta cells in type 2 diabetes - a crucial contribution to pathogenesis.Diabetes Obes Metab. 2008 May;10(5):408-20. doi: 10.1111/j.1463-1326.2007.00718.x. Epub 2007 Apr 19. Diabetes Obes Metab. 2008. PMID: 17451426 Review.
Cited by
-
Is there a role for the adaptive immune system in pancreatic beta cell failure in type 2 diabetes?Diabetologia. 2014 Mar;57(3):447-50. doi: 10.1007/s00125-013-3151-2. Epub 2013 Dec 21. Diabetologia. 2014. PMID: 24362729
-
The pore-forming subunit MCU of the mitochondrial Ca2+ uniporter is required for normal glucose-stimulated insulin secretion in vitro and in vivo in mice.Diabetologia. 2020 Jul;63(7):1368-1381. doi: 10.1007/s00125-020-05148-x. Epub 2020 Apr 29. Diabetologia. 2020. PMID: 32350566 Free PMC article.
-
Metabolic Clusters and Outcomes in Older Adults: The Cardiovascular Health Study.J Am Geriatr Soc. 2018 Feb;66(2):289-296. doi: 10.1111/jgs.15205. J Am Geriatr Soc. 2018. PMID: 29431855 Free PMC article.
-
MiRNAs in β-Cell Development, Identity, and Disease.Front Genet. 2017 Jan 11;7:226. doi: 10.3389/fgene.2016.00226. eCollection 2016. Front Genet. 2017. PMID: 28123396 Free PMC article. Review.
-
Pharmacological inhibitors of β-cell dysfunction and death as therapeutics for diabetes.Front Endocrinol (Lausanne). 2023 Mar 15;14:1076343. doi: 10.3389/fendo.2023.1076343. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37008937 Free PMC article. Review.
References
-
- Reaven GM. Role of insulin resistance in human disease. Diabetes. 1988;37:1595–1607. - PubMed
-
- Kahn SE. The relative contributions of insulin resistance and beta-cell dysfunction to the pathophysiology of type 2 diabetes. Diabetologia. 2003;46:3–19. - PubMed
-
- Maclean N, Ogilvie RF. Quantitative estimation of the pancreatic islet tissue in diabetic subjects. Diabetes. 1955;4:367–376. - PubMed
-
- Kloppel G, Lohr M, Habich K, Oberholzer M, Heitz PU. Islet pathology and the pathogenesis of type 1 and type 2 diabetes mellitus revisited. Surv Synth Pathol Res. 1985;4:110–125. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
