

Relationship between HIV coreceptor tropism and disease progression in persons with untreated chronic HIV infection
- PMID: 19194318
- PMCID: PMC2670851
- DOI: 10.1097/QAI.0b013e3181989a8b
Relationship between HIV coreceptor tropism and disease progression in persons with untreated chronic HIV infection
Erratum in
- J Acquir Immune Defic Syndr. 2009 May 1;51(1):110
Abstract
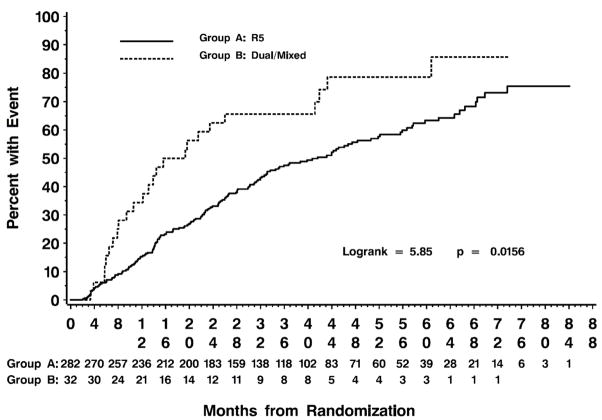
Objective: To assess the effect of HIV coreceptor tropism (CRT) on the relative risk of progression to a composite outcome of CD4 count < or =350 cells per microliter, treatment initiation, or death.
Methods: CRT assays were performed after study closure in baseline samples obtained from enrollees in a prospectively monitored cohort of treatment-naive adults with > or =450 CD4 cells per microliter and > or =1000 HIV-1 RNA copies per milliliter.
Results: Dual/mixed (D/M) and R5 CRT were detected in 32 and 282 patients, respectively. The baseline CD4 count (617 versus 694 cells/microL; P = 0.05) differed in patients with D/M versus R5 CRT. Otherwise, baseline laboratory characteristics were similar.The relative risk of progression to the composite end point was 2.15 (P = 0.002) for D/M versus R5 CRT, 2.07 per 1.0 log10 higher viral load (P < 0.001) and 0.87 per 50 cells per microliter higher CD4 cell count (P < 0.001). The effect of D/M CRT was also significant in separate analyses of time to initiation of antiretroviral therapy or CD4 cell count < or =350 cells per microliter.
Conclusions: Untreated patients with D/M rather than R5 CRT had a faster rate of disease progression, whether assessed by a composite outcome of time to CD4 count < or =350 cells per microliter, treatment initiation, or death or by separate analyses of time to CD4 count < or =350 cells per microliter or treatment initiation.
Figures
Similar articles
-
HIV replication capacity is an independent predictor of disease progression in persons with untreated chronic HIV infection.J Acquir Immune Defic Syndr. 2010 Apr 1;53(4):472-9. doi: 10.1097/QAI.0b013e3181cae480. J Acquir Immune Defic Syndr. 2010. PMID: 20032783 Free PMC article.
-
The impact of HIV tropism on decreases in CD4 cell count, clinical progression, and subsequent response to a first antiretroviral therapy regimen.Clin Infect Dis. 2008 May 15;46(10):1617-23. doi: 10.1086/587660. Clin Infect Dis. 2008. PMID: 18419499
-
Natural evolution of CD4+ cell count in patients with CD4 >350 or >500 cells/mm3 at the time of diagnosis according to HIV-1 coreceptor tropism.J Med Virol. 2012 Dec;84(12):1853-6. doi: 10.1002/jmv.23362. J Med Virol. 2012. PMID: 23080487
-
The epidemiology of HIV coreceptor tropism.Eur J Med Res. 2007 Oct 15;12(9):385-90. Eur J Med Res. 2007. PMID: 17933718 Review.
-
The role of viral coreceptors and enhanced macrophage tropism in human immunodeficiency virus type 1 disease progression.Sex Health. 2004;1(1):23-34. doi: 10.1071/sh03006. Sex Health. 2004. PMID: 16335478 Review.
Cited by
-
Efficiency of CCR5 coreceptor utilization by the HIV quasispecies increases over time, but is not associated with disease progression.AIDS Res Hum Retroviruses. 2012 Mar;28(3):289-94. doi: 10.1089/AID.2011.0006. Epub 2011 Aug 5. AIDS Res Hum Retroviruses. 2012. PMID: 21663455 Free PMC article.
-
The presence of CXCR4-using HIV-1 prior to start of antiretroviral therapy is an independent predictor of delayed viral suppression.PLoS One. 2013 Oct 1;8(10):e76255. doi: 10.1371/journal.pone.0076255. eCollection 2013. PLoS One. 2013. PMID: 24098454 Free PMC article.
-
Plasma HIV-1 Tropism and the Risk of Short-Term Clinical Progression to AIDS or Death.PLoS One. 2017 Jan 27;12(1):e0166613. doi: 10.1371/journal.pone.0166613. eCollection 2017. PLoS One. 2017. PMID: 28129343 Free PMC article.
-
Quasispecies Nature of RNA Viruses: Lessons from the Past.Vaccines (Basel). 2023 Jan 30;11(2):308. doi: 10.3390/vaccines11020308. Vaccines (Basel). 2023. PMID: 36851186 Free PMC article. Review.
-
Short Communication: A Recombinant Variant with Increased Envelope Entry Efficiency Emerged During Early Infection of an HIV-1 Subtype C Dual Infected Rapid Progressor.AIDS Res Hum Retroviruses. 2016 Mar;32(3):303-10. doi: 10.1089/AID.2014.0100. Epub 2015 May 20. AIDS Res Hum Retroviruses. 2016. PMID: 25905681 Free PMC article. Clinical Trial.
References
-
-
DHHS Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in HIV-infected adults and adolescents. February 9, 2008.
-
-
- Lyles RH, Munoz A, Yamashita TE, et al. Natural history of human immunodeficiency virus type 1 viremia after seroconversion and proximal to AIDS in a large cohort of homosexual men. Multicenter AIDS Cohort Study. J Infect Dis. 2000;181:872–80. - PubMed
-
- Learmont JC, Geczy AF, Mills J, et al. Immunologic and virologic status after 14 to 18 years of infection with an attenuated strain of HIV-1. A report from the Sydney Blood Bank Cohort. N Engl J Med. 1999;340:1715–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
