

The impact of HIV infection and CD4 cell count on the performance of an interferon gamma release assay in patients with pulmonary tuberculosis
- PMID: 19156218
- PMCID: PMC2626632
- DOI: 10.1371/journal.pone.0004220
The impact of HIV infection and CD4 cell count on the performance of an interferon gamma release assay in patients with pulmonary tuberculosis
Abstract
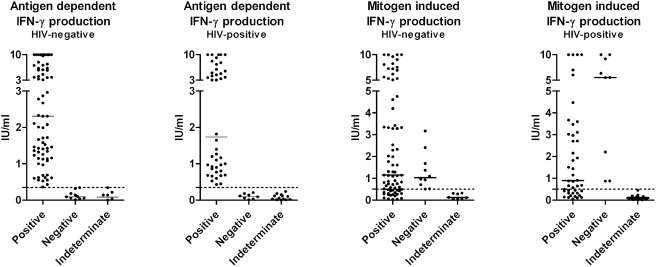
Background: The performance of the tuberculosis specific Interferon Gamma Release Assays (IGRAs) has not been sufficiently documented in tuberculosis- and HIV-endemic settings. This study evaluated the sensitivity of the QuantiFERON TB-Gold In-Tube (QFT-IT) in patients with culture confirmed pulmonary tuberculosis (PTB) in a TB- and HIV-endemic population and the effect of HIV-infection and CD4 cell count on test performance.
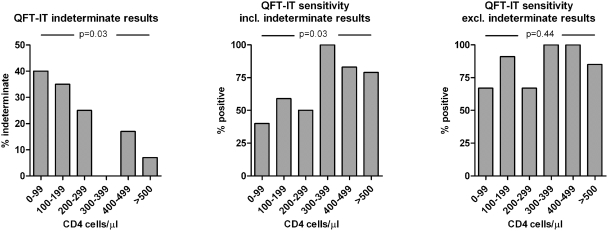
Methodology/principal findings: 161 patients with sputum culture confirmed PTB were subjected to HIV- and QFT-IT testing and measurement of CD4 cell count. The QFT-IT was positive in 74% (119/161; 95% CI: 67-81%). Sensitivity was higher in HIV-negative (75/93) than in HIV-positive (44/68) patients (81% vs. 65%, p = 0.02) and increased with CD4 cell count in HIV-positive patients (test for trend p = 0.03). 23 patients (14%) had an indeterminate result and this proportion decreased with increasing CD4 cell count in HIV-positive patients (test for trend p = 0.03). Low CD4 cell count (<300 cells/microl) did not account for all QFT-IT indeterminate nor all negative results. Sensitivity when excluding indeterminate results was 86% (95% CI: 81-92%) and did not differ between HIV-negative and HIV-positive patients (88 vs. 83%, p = 0.39).
Conclusions/significance: Sensitivity of the QFT-IT for diagnosing active PTB infection was reasonable when excluding indeterminate results and in HIV-negative patients. However, since the test missed more than 10% of patients, its potential as a rule-out test for active TB disease is limited. Furthermore, test performance is impaired by low CD4 cell count in HIV-positive patients and possibly by other factors as well in both HIV-positive and HIV-negative patients. This might limit the potential of the test in populations where HIV-infection is prevalent.
Conflict of interest statement
Figures

Similar articles
-
Interferon gamma release assays for the diagnosis of latent TB infection in HIV-infected individuals in a low TB burden country.PLoS One. 2013;8(1):e53330. doi: 10.1371/journal.pone.0053330. Epub 2013 Jan 30. PLoS One. 2013. PMID: 23382842 Free PMC article.
-
Role of interferon gamma release assay in active TB diagnosis among HIV infected individuals.PLoS One. 2009 May 28;4(5):e5718. doi: 10.1371/journal.pone.0005718. PLoS One. 2009. PMID: 19479058 Free PMC article.
-
Influential Factors of the Indeterminate Results Tested by QuantiFERON-TB Gold In-Tube (QFT-IT) Assay for Diagnosing TB Infection in HIV-Infected Patients.Clin Lab. 2016 Sep 1;62(9):1761-1766. doi: 10.7754/Clin.Lab.2016.160209. Clin Lab. 2016. PMID: 28164594
-
Interferon-γ release assays for the diagnosis of tuberculosis and tuberculosis infection in HIV-infected adults: a systematic review and meta-analysis.PLoS One. 2012;7(3):e32482. doi: 10.1371/journal.pone.0032482. Epub 2012 Mar 5. PLoS One. 2012. PMID: 22403663 Free PMC article. Review.
-
[Evolution of IGRA researches].Kekkaku. 2008 Sep;83(9):641-52. Kekkaku. 2008. PMID: 18979999 Review. Japanese.
Cited by
-
Prognostic value of indeterminate IFN-γ release assay results in HIV-1 infection.J Clin Microbiol. 2012 Aug;50(8):2767-9. doi: 10.1128/JCM.01054-12. Epub 2012 May 16. J Clin Microbiol. 2012. PMID: 22593598 Free PMC article.
-
Detection of tuberculosis in HIV-infected and -uninfected African adults using whole blood RNA expression signatures: a case-control study.PLoS Med. 2013 Oct;10(10):e1001538. doi: 10.1371/journal.pmed.1001538. Epub 2013 Oct 22. PLoS Med. 2013. PMID: 24167453 Free PMC article.
-
Joint Modeling in Detecting Predictors of CD4 Cell Count and Status of Tuberculosis Among People Living with HIV/AIDS Under HAART at Felege Hiwot Teaching and Specialized Hospital, North-West Ethiopia.HIV AIDS (Auckl). 2021 May 18;13:527-537. doi: 10.2147/HIV.S307069. eCollection 2021. HIV AIDS (Auckl). 2021. PMID: 34040450 Free PMC article.
-
QuantiFERON®-TB gold in-tube performance for diagnosing active tuberculosis in children and adults in a high burden setting.PLoS One. 2012;7(7):e37851. doi: 10.1371/journal.pone.0037851. Epub 2012 Jul 12. PLoS One. 2012. PMID: 22808002 Free PMC article.
-
Diagnostic accuracy of the interferon-gamma release assay in acquired immunodeficiency syndrome patients with suspected tuberculosis infection: a meta-analysis.Infection. 2022 Jun;50(3):597-606. doi: 10.1007/s15010-022-01789-9. Epub 2022 Mar 6. Infection. 2022. PMID: 35249210 Free PMC article. Review.
References
-
- Menzies D. Using tests for latent tuberculous infection to diagnose active tuberculosis: can we eat our cake and have it too? Ann Intern Med. 2008;148:398–399. - PubMed
-
- Diel R, Loddenkemper R, Meywald-Walter K, Gottschalk R, Nienhaus A. Comparative Performance of Tuberculin Skin Test, QuantiFERON-TB-Gold In Tube Assay, and T-Spot.TB Test in Contact Investigations for Tuberculosis. Chest 2008 - PubMed
-
- Balcells ME, Perez CM, Chanqueo L, Lasso M, Villanueva M, et al. A comparative study of two different methods for the detection of latent tuberculosis in HIV-positive individuals in Chile. Int J Infect Dis. 2008;12:645–652. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
